|
|
|
|
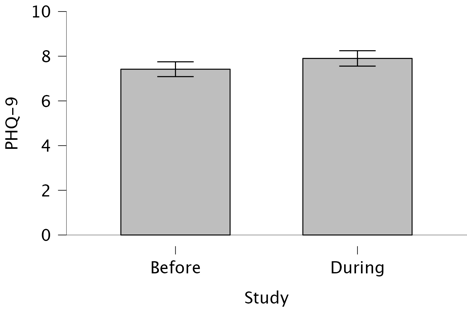
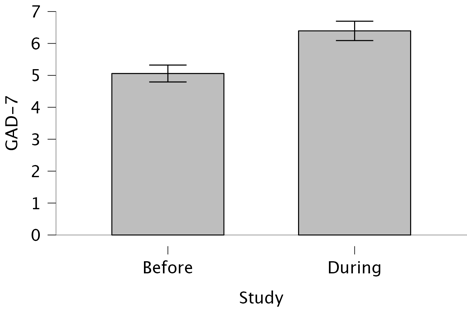
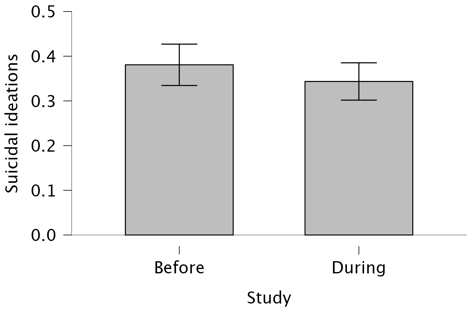
Figure 1. The severity of depressive, anxiety symptoms, and suicidal ideation in cohorts before and during the second year of the full-scale Russian invasion
Prevalence of depression, anxiety, and PTSD symptoms among patients of opioid agonist treatment programmes in Ukraine during wartime
Research article
Viktoriia Gorbunova, University of Luxembourg; Zhytomyr Ivan Franko State University, Ukraine; https://orcid.org/0000-0002-9106-3589
Vitalii Klymchuk, University of Luxembourg; National Psychological Association of Ukraine, Kyiv, Ukraine; https://orcid.org/0000-0001-7898-5530
Vladyslav Romanchuk, State Institution “Public Health Centre of the Ministry of Health of Ukraine”, Kyiv, Ukraine; https://orcid.org/0009-0009-1099-7629
Iryna Ivanchuk, State Institution “Public Health Centre of the Ministry of Health of Ukraine”, Kyiv, Ukraine
Background: The ongoing war in Ukraine has intensified psychological distress, particularly among patients receiving opioid agonist therapy (OAT). This study explores the prevalence and co-occurrence of depression, anxiety, post-traumatic stress disorder (PTSD) symptoms, and suicidal ideation among OAT patients during wartime in 2023.
Objectives: To assess the point prevalence of mental health symptoms among OAT program participants during the second year of the full-scale Russian invasion of Ukraine, and to compare these findings with pre-war baseline data.
Methods: A descriptive cross-sectional study was conducted using standardized screening tools (GAD-7, PHQ-9, and PCL-5) to measure symptoms among patients across OAT centres in Lviv, Sumy, and Vinnytsia between April and October 2023. Additional measures included missed visits and dose satisfaction over the past month. The data were compared to pre-invasion data collected from October 2021 to January 2022 in Kyiv, Sumy, and Lviv.
Results: Among the screened population, 17.43% reported concurrent depressive, anxiety, and PTSD symptoms. Females exhibited higher depressive symptoms (45.26%) compared to males (31.28%). Patients on buprenorphine showed a higher prevalence of suicidal ideation (33.96%) and PTSD symptoms (44.96%) than those on methadone (22.64% and 31.1%, respectively). The mean trauma exposure was 4.11 events per person. A significant increase in depression (mean PHQ-9 score from 7.42 to 7.90) and anxiety (mean GAD-7 from 5.06 to 6.39) was observed, alongside an increase in probable depression (from 26.73% to 32.62%) and generalized anxiety (from 14.72% to 25.51%). Suicidal ideation rates remained largely unchanged.
Conclusions: The findings highlight the compounding mental health burden among OAT patients during wartime and underscore the urgent need to embed psychosocial support services within OAT programs to enhance patient well-being and societal reintegration.
Keywords: opioid agonist therapy (OAT), mental health, depression, anxiety, suicidal ideation, PTSD.
Introduction
The relationship between opioid use and other mental health conditions has been explored and well-documented. The DSM-5-TR highlights the frequent comorbidity of opioid-related disorders with other substance use, depressive disorders, both induced and independent, sleep disorders, PTSD, bipolar I and separate personality disorders, etc. (APA, 2022). Alongside mental disorders, there is an increased risk of suicidal thoughts and behaviour, in particular through severe depression (APA, 2022, P. 614). The symptoms and disorders can be either induced by substance use, be pre-existing, or mediated through a third mental or physical condition.
Opioid agonist therapy (OAT, providing substitute medications for people with opioid use disorder), in addition to HIV / hepatitis prevention and other physical health advantages, also benefits the socialisation and emotional stability of committed patients. That is why consistent epidemiological data on the mental health of OAT programme participants are essential. Depression and anxiety are the two most commonly evaluated mental conditions for OAT patients, and they often show higher prevalence numbers than in the general population. Although research indicates that prevalence rates for depression and anxiety among OAT patients vary widely, ranging from about 50% to 20%, there is a lack of data from the countries going through the war and humanitarian crises (Aas et al., 2020; Iskandar et al., 2013; Roncero et al., 2016; Rosic et al., 2021; Teoh Bing Fei et al., 2016; Wu et al., 2013).
Even though initiation of the opioid agonist treatment is associated with a reduced risk of self-harm, it is not significantly related to the risk of suicide: the mortality ratio for suicide is 7,5 times higher in OAT patients in comparison with the non-sampled population (Padmanathan et al., 2022). As for suicidal ideation, patients receiving OAT for opioid-use disorder more often (starting from around 20%), which is twice as much as in the general population, report related thoughts with their increase in two to four times in cases with psychiatric comorbidity, early onset of substance use, history of overdose (Rosic et al., 2021; Andersson et al., 2022; Au et al., 2021; Pant et al., 2022; Vold et al., 2022).
Posttraumatic stress disorder symptoms were found in 11% - 35% of methadone maintenance treatment patients (Rosic et al., 2021; Applebaum et al., 2010; Barry et al., 2011; Engstrom et al., 2012; Himelhoch et al., 2012; Rosen et al., 2008; Villagonzalo et al., 2011). Furthermore, the presence of mental health comorbidities has been linked to poorer treatment adherence, less favourable treatment outcomes, more severe opioid use patterns, and increased mortality rates in patients treated with substitution medications (Huang & Lee, 2013; Ngo et al., 2011; Peles et al., 2006; Rosic et al., 2017).
Our previous study of some mental health characteristics of OAT patients in Ukraine shows symptoms’ prevalence from moderate to severe in 26.73% of cases for depression, 14.71% for generalised anxiety and 24.9% for 2-week suicidal ideation, which is comparable with other vulnerable populations in Ukraine, e.g. Romani people or internally displaced persons, but much higher than in general population (Klymchuk et al., 2024).
The Russian full-scale invasion of Ukraine caused massive destruction and devastation, leading to the deterioration of the mental health of many Ukrainians. Data from recent wartime studies on the Ukrainian sample show an increase in the prevalence of war-related PTSD in all age groups, as well as anxiety and depression symptoms, as self-reported by adults (McElroy et al., 2024; Karatzias et al., 2023; Hyland et al., 2023). Taking into account the WHO estimations that one in five people (22%) who have been through a war or other conflict will have depression, anxiety, post-traumatic stress disorder, bipolar disorder, or schizophrenia (Charlson et al., 2019), we expect that the prevalence of mental health symptoms among Ukrainian OAT programme participants will increase in wartime.
This research aims to explore the prevalence of depressive, anxiety, PTSD symptoms, suicidal ideation, and their co-occurrence among the patients of the OAT programs in Ukraine during the second year (April to October 2023) of the full-scale Russian invasion of Ukraine. The main research objectives were: to measure the severity and prevalence of depressive, anxiety, PTSD symptoms, and suicidal ideation; to assess the co-occurrence of depressive, anxiety, and PTSD symptoms; to compare the severity and prevalence of the symptoms across groups based on gender, age, and the type of substitute medications; to explore the relationship between symptom prevalence, dosage satisfaction, and missed doses; and to compare the prevalence of the symptoms before and during the full-scale Russian invasion of Ukraine.
Materials and Methods
Study design. The study was organised using a descriptive cross-sectional design with one-time point (point prevalence) measurement of depressive, generalised anxiety, posttraumatic stress disorder (PTSD) symptoms, and suicidal ideation of OAT patients, together with the estimation of a number of missed visits on-site to receive substitute medication and dose satisfaction for the last month. The data report follows the Observational Studies in Epidemiology (STROBE) Statement.
Setting. All the data were collected based on opioid agonist therapy centres in three Ukrainian cities: Vinnytsia (Central part of Ukraine), Sumy (Eastern part of Ukraine), and Lviv (Western part of Ukraine) from April to October 2023 (after the full-scale Russian invasion). The staff of OAT centres have collected all the data. Doctors, psychologists, or social workers who had previously obtained detailed instructions performed individual screenings during patients’ appointments. The questionnaires were printed out and filled in together with each patient.
Participants. The study engaged all the patients of the defined OAT centres who were receiving substitute medications during the data collection period. Recruitment and data collection period: from April to October 2023. All participants were informed of the study’s purpose, including its potential to inform service improvements and individualised care. All participants could receive on-site psychological support after the data collection. Informed consent was obtained from all participants.
Variables. Among studied outcomes are the severity of depressive, anxiety and PTSD symptoms according to DSM-diagnostic criteria for major depressive disorder, generalised anxiety disorder and posttraumatic stress disorder, respectively, as well as the presence of suicidal ideation as thoughts of “would be better off dead, or thoughts of hurting yourself in some way”. Possible outcome predictors are the number of missed visits on-site to receive substitute medication, dose satisfaction for the last month, the gender and age of the participants, and the type of substitute medication (methadone, buprenorphine, or buvidal). Staying in Ukraine during the second year of the full-scale Russian invasion of Ukraine is considered an exposure variable.
Data sources/measurement. For the measurement of the primary outcomes, we used a set of DSM-based self-reporting scales: PHQ-9 for depression symptoms, the 9th question separately for suicidal ideation, GAD-7 for anxiety symptoms, PCL-5 for PTSD symptoms, accompanied by LEC-5 event list for the screening of traumatic exposure. In addition, the number of missed visits on-site for substitute medication for the last month was counted, and satisfaction with the dose was recorded. Satisfaction with the dose of the medication was assessed using the question: “What is your satisfaction level with the dosage of your medication (from 1 to 10, with 10 – maximum satisfaction)?”. The data were compared to the ones previously collected (before the full-scale Russian invasion, 10.2021-01.2022, Kyiv, Sumy, and Lviv).
Bias. All the patients of the defined OAT centres were screened to prevent selection bias. Individually guided screening by medical staff and social workers (not self-administration of the scales) was employed to reduce the effect of non-response and measurement biases.
Statistical methods. Data analysis and visualisation were performed using JASP 0.14.3 (GNU Affero GPL v3 license, an open-source license). Descriptive statistics (mean, standard deviation, frequency analysis) were used to describe the general results. The Nonparametric Kruskal-Wallis one-way ANOVA was used to analyse multiple differences between independent samples with Dunn’s post-hoc test. The Shapiro-Wilk test was used to analyse the normality of distributions. The contingency tables were used to analyse the co-occurrence of mental health conditions. The nonparametric Mann-Whitney U-test was utilised to examine differences between data collected before and during (the second year) the full-scale Russian invasion of Ukraine.
Results
Participants
The overall sample consisted of 984 OAT centres’ patients from Vinnytsia, Sumy, and Lviv; all of them were screened with PHQ-9 and GAD-7 for assessing depressive, generalised anxiety symptoms, and suicidal ideation. Of them, 376 participants refused to answer the questions about trauma experience using the possibility of voluntary participation in trauma screening, so only 608 persons went through the LEC-5 event list for the screening of traumatic exposure, and 549 of them (those who had experienced at least one traumatic event) were examined with PCL-5 for PTSD symptoms screening. Among study participants (95 females and 889 males), 347 OAT centres’ patients were from Vinnytsia, 313 were from Lviv, and 324 were from Sumy (Table 1). The mean age for participants was 40.9: 41.4 for females and 40.8 for males (Table 2). Regarding the medications, 8 patients, all males, were receiving Buvidal, 212 (191 males, 21 females) – Buprenorphine, and the biggest share of 764 patients (690 males, 74 females) were on Methadone (Table 3).
Table 1. Sample description (gender, location)
|
Location |
Females |
Males |
Total |
||||||
|
Vinnytsia |
Count |
33 |
314 |
347 |
|||||
|
% within row |
9.510 % |
90.490 % |
100 % |
||||||
|
% within column |
34.737 % |
35.321 % |
35.264 % |
||||||
|
Lviv |
Count |
38 |
275 |
313 |
|||||
|
% within row |
12.141 % |
87.859 % |
100 % |
||||||
|
% within column |
40 % |
30.934 % |
31.809 % |
||||||
|
Sumy |
Count |
24 |
300 |
324 |
|||||
|
% within row |
7.407 % |
92.593 % |
100 % |
||||||
|
% within column |
25.263 % |
33.746 % |
32.927 % |
||||||
|
Total |
Count |
95 |
889 |
984 |
|||||
|
% within row |
9.654 % |
90.346 % |
100 % |
||||||
|
% within column |
100 % |
100 % |
100 % |
||||||
Table 2. Sample description (age, gender)
|
95% Confidence Interval Std. Dev. |
|||||||||||||||||||||||
|
Valid |
Missing |
Mean |
Std. Deviation |
Upper |
Lower |
Shapiro-Wilk |
P-value of Shapiro-Wilk |
Minimum |
Maximum |
||||||||||||||
|
Females |
95 |
0 |
41.347 |
7.399 |
8.675 |
5.933 |
0.949 |
< .001 |
25 |
66 |
|||||||||||||
|
Males |
889 |
0 |
40.785 |
6.770 |
7.165 |
6.358 |
0.975 |
< .001 |
18 |
74 |
|||||||||||||
|
|
|
All |
|
984 |
|
0 |
|
40.839 |
|
6.831 |
|
7.257 |
|
6.436 |
|
0.973 |
|
< .001 |
|
18 |
|
74 |
|
Table 3. Sample description (type of substitute medication, location, gender)
|
|
Buvidal |
Buprenorphine |
Methadone |
Total |
|||||
|
Location |
Vinnytsia |
0 |
72 |
275 |
347 |
||||
|
Lviv |
5 |
89 |
219 |
313 |
|||||
|
Sumy |
3 |
51 |
270 |
324 |
|||||
|
Gender |
Females |
0 |
21 |
74 |
95 |
||||
|
Males |
8 |
191 |
690 |
889 |
|||||
|
Total |
8 |
212 |
764 |
984 |
|||||
To analyse the prevalence of the symptoms before and during (the second year) of the full-scale Russian invasion of Ukraine, data collected in 2023 were compared with the data from a similar sample of 999 participants who were screened with PHQ-9 and GAD-7 from October 2021 to January 2022 (before the full-scale Russian invasion) based on OAT centres in Kyiv, Sumy and Lviv (Klymchuk et al., 2024). Two centres (Sumy and Lviv) are the same as in the current study, and one (Kyiv) is different. It was changed to Vinnytsia centre (also from the central part of Ukraine) due to the staff overload and, therefore, the inability to participate in the research (Table 4).
Table 4. Location of the study participants (cohorts studied before the full-scale Russian invasion of Ukraine and in the second year of the invasion)
|
Before the full-scale Russian invasion |
During the second year of the full-scale Russian invasion |
||||
|
Location |
N |
Percent |
Location |
N |
Percent |
|
Kyiv |
354 |
35.4% |
Vinnytsia* |
347 |
35,2% |
|
Lviv |
337 |
33.7% |
Lviv |
313 |
31,9% |
|
Sumy |
308 |
30.8% |
Sumy |
324 |
32,9% |
|
Total |
999 |
100% |
Total |
984 |
100% |
|
* Replacement of the location (Vinnytsia instead of Kyiv) |
|||||
Severity and prevalence of depressive, anxiety, PTSD symptoms, and suicidal ideation
Cumulative averages for all measurements showed no significant extremums (Annex, Table 5). Here and further Annexes can be found in Klymchuk (2025). The average GAD-7 score is 6.39 (bottom line for mild anxiety), the average PHQ-9 score is 7.9 (mild depression), and the PTSD score is 24.43 (no PTSD). None of the distributions complied with the normal distribution criteria (Shapiro-Wilk test).
For calculations of the frequency of individual trauma exposure, we used the LEC-5 event list, asking participants if each event happened to them or was witnessed by them. The average exposure was 3.06 “happened to me” events (maximum 16 events per 1 person) and 1.05 “witnessed” events (maximum 10 events per person). The overall rate of trauma exposure (“happened to me” plus “witnessed” events) was 4.11 events per person (Annex, Table 6).
Depressive symptoms from moderate to severe levels were found in 32.62% of cases (severe – 2.85%, moderately severe – 11.38%, moderate – 18.39%) (Annex, Table 7). The cut-off score for clinical significance of PHQ-9 measurements for probable major depressive disorder (MDD) is 10 (Manea & McMillan, 2012).
Moderate to severe generalised anxiety symptoms were reported by 25.50% of participants (severe – 7.11%, moderate – 18.39%) (Annex, Table 8). The cut-off score of 10 is considered clinically significant for probable generalised anxiety disorder (GAD) (Spitzer et al., 2006).
The 2-week suicidal ideation prevalence as the occurrence of related thoughts at least several days per two-week time is 25.01% of all OAT patients who participated in the screening (several days – 17.28%, more than half the days – 6.1%, nearly every day – 1.63%) (Annex, Table 9).
Data on trauma exposure reveal that 90.3% (549 out of 608) of the patients subjected to LEC-5 event list screening had experienced at least one traumatic event (Annex, Table 10).
PTSD prevalence (1 month) was calculated using a recommended PCL-5 cut-off score of 31 for probable PTSD (Forkus et al., 2023). Screening was applied only to those who had trauma exposure, according to LEC-5. More than 1/3 (34.43%) of participants who experienced at least one trauma event were screened positive for so-called “probable PTSD” (Annex, Table 11).
Co-occurrence of depressive, anxiety, and PTSD symptoms
To analyse the co-occurrence of mental health conditions, contingency tables were used with the same recommended cut-off scores for each scale (Annex, Table 12). 24.5% of OAT patients (149 out of 608 screened participants) had both probable PTSD and major depressive disorder, in 19.08% of cases (116 out of 608) were found simultaneous probable PTSD and generalised anxiety disorder (GAD), and data 22.56% of participants (222 out of 984) showed cooccurrence probable GAD and major depressive disorder.
The contingency table for the sample screened with all the scales (n=608) showed that three types of symptoms are present in 17.43% (106) of OAT patients (Annex, Table 13).
Severity and prevalence of the symptoms across groups based on gender, age, and the type of substitute medications
The mean levels for depressive, anxiety, PTSD symptoms, and suicidal ideation in females are higher than in males (Annex, Table 5); however, only differences for PTSD symptoms (females – 28.42, SD 16.56; males – 23.91, SD 16.4) are statistically significant (p=0.016) according to non-parametric Mann-Whitney U Test which was utilised due to the data deviation from the normal distribution (Shapiro-Wilk criteria) (Annex, Table 14).
The same tendency, with higher numbers for females than males, works for depression, anxiety, PTSD symptoms, and suicidal ideation prevalence (Annex, Tables 7-9, 11). As for statistical significance, only a 2-week prevalence of depressive symptoms (females – 45.26% (severe 5.26% + moderately severe 10.53% + moderate 29.47%), males – 31.28% (severe 2.6% + moderately severe 11.47% + moderate 17.21%)) were found significantly different (p=0.019) between female and male groups based on the Chi-Squared Test (Annex, Table 15).
Differences in the severity of the mental symptoms among persons receiving different OAT medications (methadone, buprenorphine, or buvidal) are presented in Annex, Tables 6-8 and 10. To analyse their statistical significance, we used non-parametric ANOVA (Kruskal-Wallis test) (Annex, Table 16). As there were not enough data on buvidal to make conclusions (only 8 patients were receiving it), they were excluded from the analysis. There were no significant connections between the type of OAT medication and the severity of mental health symptoms, except for suicidal ideation (p=0.003), with significantly higher numbers for the severity of the symptoms for the patients on Buprenorphine (0.46, SD 0.7) over the patients on Methadone (0.31, SD 0.65).
Additionally, Dunn’s post hoc comparison revealed a significant difference (p=0.027) in the severity of PTSD symptoms between patients receiving buprenorphine (27.19; SD 17.14) and methadone (23.56; SD 16.08). A highly significant difference (p<0.001) was observed for suicidal ideation, with patients receiving buprenorphine exhibiting more severe levels of suicidal ideation (0.46; SD 0.7) compared to those on methadone (0.31; SD 0.65) (Annex, Table 17).
Regarding the prevalence, significant differences were observed between patients using methadone and buprenorphine for suicidal ideation (p<0.001) and PTSD symptoms (p = 0.014) (Annex, Table 18). Share of the patients with suicidal ideation using methadone was 22.64% (several days 16.1% + more than half the days 4.58% + nearly every day 1.96%), buprenorphine – 33.96% (several days 22.17% + more than half the days 11.79% + nearly every day 0%); PTSD symptoms were found in 44.96% patients on Buprenorphine and 31.1% of methadone patients.
The differences must be perceived as exploratory and preliminary, as the sample size and data structure do not support robust multivariable modelling without risking overfitting or unstable estimates.
Conclusions regarding buvidal are impossible to make due to the size of the sample (only 8 participants were receiving this medication).
No connections between age and studied mental symptoms of the OAT patients were revealed during correlation analyses (non-parametric Spearman rho coefficient due to the data deviation from the normal distribution) (Annex, Table 19).
Relationship between symptom prevalence, dosage satisfaction, and missed doses
Table 20 (Annex) provides data on patient dose satisfaction and missed doses. The mean satisfaction with the prescribed dose is 8.55 (SD 1.51) out of 10. The mean missed doses due to skipped visits on-site during the last month is 0.38 (SD 1.11).
The results of the correlation analysis between dose-related parameters and mental symptoms of the OAT patients are presented in Annex, Table 21. There are no significant correlations between dose satisfaction and suicidal ideation as well as PTSD symptoms (in both cases, p>0,05). Small but significant negative correlations were found between dose satisfaction and symptoms of depression (-0.21; p<0.001), dose satisfaction and symptoms of generalised anxiety (-0.19; p<0,001). Missed on-site visits and suicidal ideation are correlated at the level of 0.23 (p<0.001), depressive symptoms (0.44; p<0.001), and generalised anxiety symptoms (0.42; p<0.001). The correlation between missed doses and PTSD symptoms is insignificant.
Prevalence of the symptoms before and during (the second year) of the full-scale Russian invasion of Ukraine
Descriptive statistics before the full-scale Russian invasion (Klymchuk et al., 2024) are presented in Annex, Table 22; results of the Mann-Whitney U tests for the significance of the differences are in Annex, Table 23.
The severity of depressive symptoms increased significantly from 7.42 (SD 5.34) before the full-scale Russian invasion to 7.90 (SD 5.51) during the second year of the full-scale Russian invasion (p<0,05); the same tendency is observed for the generalised anxiety symptoms severity – it increases significantly (p<0.001) from 5.06 (SD 4.26) to 6.39 (SD 4.85). No significant changes were seen in suicidal ideation, p>0.05, Figure 1 (Annex, Tables 5, 22-23).
|
|
|
|
Figure 1. The severity of depressive, anxiety symptoms, and suicidal ideation in cohorts before and during the second year of the full-scale Russian invasion
Absolute change revealed, despite statistical significance, is below typical clinically important difference thresholds.
As for the changes in the prevalence, significant differences were found for depressive and generalised anxiety symptoms, which grew from 26.73% to 32.62% (p<0,001) and from 14.72% to 25.51% (p<0,001), respectively, when suicidal ideation didn’t change significantly (Annex, Tables 24-25).
Discussion
At the beginning of the full-scale Russian invasion, there was a disruption in the daily work of OAT centres in Ukraine and patients’ treatment routine due to patients’ displacement, shortage of medication supply, safety issues, etc. In time, OAT centres established specific procedures and practices of care to cope with persistent war-related circumstances, such as electricity shortages or shelling, and secured medication stock. The OAT centres involved in the study entered the second year of the invasion with established processes that allowed them to participate in research without overwhelming the medical staff and while adhering to the methodology.
Prevalence of depressive, anxiety, PTSD symptoms, and suicidal ideation
The results of the study revealed a substantial prevalence of depressive, anxiety, and PTSD symptoms, as well as suicidal ideation among patients receiving OAT in specialised centres in Ukraine during the second year of the full-scale Russian invasion.
Depressive symptoms were found in 32.62% of study participants, and generalised anxiety symptoms in 25.50%. These data are comparable with data from other countries collected based on OAT clinics with a similar methodology and identical cut-off scores for PHQ-9 and GAD-7 -screening scales: Canada (MDD - 28.22%; GAD - 19.63%), Malaysia (MDD - 30.6%), India (MDD - 30.5% GAD - 39%), and USA (MDD - 23.3%; GAD - 23.2%) (Rosic et al., 2017; Saad et al., 2021; Rathi et al., 2024; Amura et al., 2022).
The prevalence of depression in Ukraine found in other studies is higher both in small and large samples. Thus, 43.5% of 4421 patients enrolled on OAT across 12 specialised centres were screened with MDD; 49,9 % of 1345 patients maintained on medications for opioid use disorder at 12 OAT centres had signs of moderate/severe depression; 56% of 187 people who live with HIV and inject drugs were scored with 10 or above with PHQ-9 (Machavariani et al., 2023; Morozova et al., 2023; Zeziulin et al., 2021). However, the high numbers in the last case can be explained by the specificity of the sample, as only around half of the participants reported currently or previously being on OAT (Zeziulin et al., 2021).
The Ukrainian sample of injectable drug users with HIV showed 26% prevalence of suicidal thoughts (Zeziulin et al., 2021), which is close to 25.01% 2-week suicidal ideation prevalence in our research. In general, 20-30 % is a typical frame for 2-week, month, and even lifetime prevalence of suicidal ideation in the studied population, with an increase among those who reported recent overdose, having a comorbid mood, anxiety, psychotic, or personality disorder, and cannabis use (Au et al., 2021; Pant et al., 2022; Rosic et al., 2020; Archambault et al., 2022; Naji et al., 2021).
The overall rate of trauma exposure among our study participants was 4.11 events per person, with 34.43% of the prevalence of PTSD symptoms. Such a prevalence number is very close to or slightly higher than in similar studies on different age, sex, and race samples in other countries (Engstrom et al., 2012; Rosen et al., 2008; Rosic et al., 2017; Peck et al., 2021; Trafton et al., 2006; Kumari et al., 2016; Becker et al., 2015).
Co-occurrence of depression, anxiety, PTSD symptoms, and suicidal ideation
The presence of triadic symptomatology (depression, anxiety, and PTSD) was found in 17.43% of studied OAT patients. A quarter of our patients (24.5%) had both PTSD and major depressive disorder symptoms, 19.08% of them showed both symptoms of PTSD and generalised anxiety, and 22.56% of participants exhibited co-occurrence of probable generalised anxiety and major depressive disorders. Such comorbidity reflects a shared aetiology (Smoller, 2016), possibly exacerbated by the current war circumstances, and highlights the complexity of mental health challenges in this population. Thus, 60-80% and more of OAT patients had at least one comorbid psychiatric disorder, with the biggest share for anxiety, mood, and sleep disorders (Roncero et al., 2016; Rosic et al., 2017; Morin et al., 2020).
Severity and prevalence of the symptoms across groups based on gender, age, and the type of substitute medications
In the current study, gender-based differences in the severity and prevalence of PTSD symptoms were found to be statistically significant, with females reporting higher levels of PTSD than males (females – 28.42, SD 16.56; males – 23.91, SD 16.4). Among persons treated for opioid use disorder, females are more likely to have PTSD (Rosic et al., 2021; Saraiya et al., 2024).
Gender differences for the severity of depressive and anxiety symptoms, yet present, were found not significant, and that does not resonate with previous big sample research demonstrating that women from the general population, particularly those exposed to trauma (in our sample, 90.3% of the patients subjected to LEC-5 event list screening had experienced at least one traumatic event), are significantly likely to have more severe depression or GAD than men (Roberts et al., 2020; Preti et al., 2021). One possible explanation for the insignificance of the obtained results is our sample's predominance of male participants. However, the 2-week prevalence of depressive symptoms (females – 45.26%, males – 31.28%) was found to be significantly higher in women, which might be connected with the issue of the challenges (hormonal factors, prevalence of trauma experience, stigma) women face entering treatment for opioid use disorder (Huhn & Dunn, 2020).
The type of substitute medication, specifically methadone and buprenorphine, was significantly associated with the severity and prevalence of suicidal ideation and PTSD symptoms in our research. Patients on buprenorphine showed significantly higher levels of suicidal ideation (0.46; SD 0.7) and PTSD symptoms (27.19; SD 17.14) compared to those on methadone (0.31; SD 0.65 and 23.56; SD 16.08 retrospectively). The same tendency in terms of the significance of the differences was revealed for the prevalence; 33.96% of patients using buprenorphine reported suicidal ideation, and 44.96% of patients had PTSD in comparison with 22.64% and 31.1% of methadone patients.
These findings warrant further investigation into how different opioid substitution medications might influence mental health, especially in light of mixed data on the effectiveness of buprenorphine in treating depression and PTSD and reducing suicidal behaviour (Madison & Eitan, 2020; Serafini et al., 2018; Meshberg-Cohen et al., 2021).
Relationship between symptom prevalence, dosage satisfaction, and missed doses
Those of our participants who reported dissatisfaction with their OAT dosages experienced higher levels of depression (-0.21; p<0.001) and anxiety (-0.19; p<0,001) symptoms. Also, missed doses were positively correlated with suicidal ideation (0.23; p<0.001), depressive (0.44; p<0.001), and generalised anxiety symptoms (0.42; p<0.001). Our findings align with other data from Ukraine on correlates of depression, which, among others, are higher methadone dosages, internalised stigma, and low trust in physicians (Morozova et al., 2024).
There is also data that OAT patients are less likely to report being unsatisfied with their dose if they have worse psychological health (according to MAP Psychological Health Score) or have ever attempted suicide (Beaumont et al., 2024), report lesser levels of personal functioning and well-being (Alcaraz et al., 2018), have more psychological symptoms (based on Maudsley Addiction Profile) (Marchand et al., 2011) or high level of depression (Hassan et al., 2023).
Severity and prevalence of depressive, anxiety, PTSD symptoms, and suicidal ideation among patients of OAT centres in Ukraine before full-scale Russian invasion and during the second year of invasion
The comparison of the symptoms’ severity and prevalence indicates a significant deterioration in the mental health of OAT patients in Ukraine during the second year of the full-scale Russian invasion. The escalation of depressive (from 7.42; SD 5.34 to 7.90; SD 5.51) and anxiety symptoms (from 5.06; SD 4.26 to 6.39; SD 4.85), as well as the increase in prevalence from 26.73% to 32.62% for probable depression and from 14.72% to 25.51% for probable generalised anxiety in the context of ongoing war, mirrors the findings of other studies in the war zone in Ukraine on different samples, where the chronic stress of war leads to heightened mental health problems (McElroy et al., 2024; Karatzias et al., 2023; Hyland et al., 2023).
As for the particular impact of the Russian full-scale invasion on OAT programs in Ukraine, there are constant concerns about the availability, dosage, and quality of OAT, as well as difficult access to the programs for specific groups, such as refugees or patients living under the occupation (Dubov et al., 2024). The mentioned and other difficulties are not factors that improve the mental health of the patients.
One more study result is worth mentioning separately – the absence of any change in suicidal ideation. This finding aligns with existing literature suggesting that suicidality may not peak during active conflict, but rather in its aftermath. Wartime conditions, characterised by heightened survival focus, social cohesion, and restricted access to means, may temporarily suppress suicidal thoughts. Historical analyses of U.S. military suicide rates, for example, indicate lower rates during major wars, with increases observed in post-conflict periods (Smith et al., 2019). Similarly, post-war studies in different countries highlight the role of cumulative stressors, such as displacement, bereavement, and economic instability, in driving suicidality after hostilities cease (Lester, 1994; Karam et al., 2012; Amone-P’Olak, 2014).
These insights underscore the importance of longitudinal monitoring and post-war mental health planning for OAT populations in Ukraine and other conflict-affected regions.
War significantly impacts people's wellbeing and mental health; that is especially true for vulnerable populations, among whom there are people with substance use disorders. Uninterrupted service delivery for those receiving OAT might be a protective factor, providing them with complex support. However, even resilient healthcare services cannot provide complete mental health protection in the face of such prolonged exposure to the atrocities of war.
It was found that there was a significant escalation of depressive (from 7.42; SD 5.34 to 7.90; SD 5.51) and anxiety symptoms (from 5.06; SD 4.26 to 6.39; SD 4.85), as well as an increase in prevalence from 26.73% to 32.62% for probable depression and from 14.72% to 25.51% for probable generalised anxiety. The overall rate of trauma exposure was 4.11 events per person, with 34.43% of the prevalence of PTSD symptoms (among those who were tested). However, the suicidal ideation rate didn`t increase at all (25,33% before and 25% during the full-scale invasion).
Such results, alongside other findings (high level of co-occurrence of depressive, anxiety and PTSD symptoms (17,43%); increased prevalence of depressive symptoms in females (45.26% vs 31.28%); increased prevalence of suicidal ideations in patients receiving buprenorphine (33.96% vs 22.64% for methadone) and increased prevalence of PTSD symptoms among those patients (44.96% vs 31.1% for methadone)) point out the need for further development of psychosocial support services, integrated into the work of OAT centres and potentially transforming them into community-based mental health and psychosocial centres. Such integration can improve mental health outcomes for OAT patients, providing them with much-needed support in a consistent way and supporting their reintegration and inclusion into society.
Such recommendations for both clinical practice and policy development are proposed:
-Integrating routine mental health screening (e.g., PHQ-4, LEC-5, PCL-5) into OAT programmes, especially during periods of heightened stress such as armed conflict.
-Training OAT staff in trauma-informed care, including brief psychosocial interventions to improve patient engagement and reduce screener refusal rates.
-Establishing referral pathways for patients with elevated symptoms of depression, anxiety, or PTSD to receive timely psychological support.
-Advocating for policy-level support to ensure mental health resources are embedded within addiction treatment services, particularly in conflict-affected regions.
Limitations of the study:
The study has several limitations. The stage of the OAT treatment was not recorded for each patient; therefore, it is impossible to draw a conclusion on the impact of the OAT lengths and stage on the patient’s mental health condition.
This study's data collection geography differs from the previous one (04-10.2023: Vinnytsya, Sumy, Lviv; 10.2021-01.2022: Kyiv, Sumy, and Lviv). Specifically, Kyiv was included in the pre-war sample but replaced by Vinnytsia in the wartime wave due to logistical constraints. The substitution of Kyiv with Vinnytsia may have introduced site-level variation in patient characteristics and service delivery. As such, observed differences in mental health outcomes between cohorts may reflect both temporal changes and differences in case-mix.
Data collection occurred in different seasons (October–January vs April–October), which may influence mood and anxiety levels. Additionally, gender proportions and OAT medication types may vary between cohorts. Findings should be interpreted as associations rather than causal effects, and future research should employ fully adjusted models with consistent site sampling and seasonal controls.
Trauma and PTSD data were collected in 2/3 of the patients screened for Depression and Anxiety, and the other 1/3 refused to fill in the LEC-5 and PCL-5 screeners, so PTSD prevalence might be underestimated due to the assumption that refusal came from the people with the highest trauma experience. Therefore, it is impossible to make reliable conclusions on PTSD prevalence. There is also asymmetry in the gender distribution of study participants, which can impact the conclusions drawn.
Screening was interviewer-administered by clinic staff, which posed the risks of social desirability and interviewer bias, particularly in the reporting of sensitive symptoms such as suicidal ideation. Participants may have underreported distress due to perceived stigma or fear of judgment. To mitigate these risks, screenings were conducted in private settings using a standardised script. However, a self-administration option was not offered, which may have limited disclosure. Future studies should consider incorporating anonymous or self-administered formats to enhance data validity, especially for high-stigma indicators.
Ethical statement:
The study protocol was developed in close collaboration with representatives of the OAT sites. Experts from the OAT sites evaluated all research tools. The research team adhered to the Declaration of Helsinki and the National Psychological Association of Ukraine Ethical Regulation. All the research stages were developed according to the requirements of international guidelines for the ethical review of epidemiological studies. The Study Protocol was approved by the Institutional Review Board of the State Institution “Public Health Centre of the Ministry of Health of Ukraine“, approval N 326.
Data availability statement:
Data supporting these findings are available within the article or upon request made to the State Institution “Public Health Centre of the Ministry of Health of Ukraine” according to approved procedures outlined at the Centre’s website: https://phc.org.ua/naukova-diyalnist/doslidzhennya.
The Annex is available via Zenodo (Klymchuk, 2025).
Funding:
The article is based on the results of the study performed by the State Institution “Public Health Centre of Ministry of Health of Ukraine” within the program of the Global Fund to Fight AIDS, Tuberculosis and Malaria, “Accelerating Progress in Reducing the Burden of Tuberculosis and HIV Infection in Ukraine”, in accordance with the Grant Agreement between the Public Health Centre of Ministry of Health of Ukraine and the Global Fund to Fight AIDS, Tuberculosis and Malaria No. 1936 of December 04, 2020. The donor was not involved in the study design, the collection, analysis, and interpretation of data, or the preparation of the article. No funding was received for the article preparation/submission/APC.
Competing interests:
The authors declare no competing interests.
Acknowledgement:
The authors want to express their sincere gratitude to all study participants, OAT patients, and staff members. Without their support and dedication, it would be impossible to conduct this study.
References:
Aas, C. F., Vold, J. H., Skurtveit, S., Lim, A. G., Ruths, S., Islam, K., et al. (2020). Health-related quality of life of long-term patients receiving opioid agonist therapy: A nested prospective cohort study in Norway. Substance Abuse Treatment, Prevention, and Policy, 15, 1–12. https://doi.org/10.1186/s13011-020-00309-y
Alcaraz, S., Viladrich, C., Trujols, J., Sinol, N., & Perez de los Cobos, J. (2018). Heroin-dependent patient satisfaction with methadone as a medication influences satisfaction with basic interventions delivered by staff to implement methadone maintenance treatment. Patient Preference and Adherence, 12, 1203–1211. https://doi.org/10.2147/PPA.S164181
Amone-P’Olak, K., Lekhutlile, T. M., Meiser-Stedman, R., & Ovuga, E. (2014). Mediators of the relation between war experiences and suicidal ideation among former child soldiers in Northern Uganda: The WAYS study. BMC Psychiatry, 14(271). https://doi.org/10.1186/s12888-014-0271-2
Amura, C. R., Sorrell, T. R., Weber, M., Alvarez, A., Beste, N., Hollins, U., et al. (2022). Outcomes from the medication assisted treatment pilot program for adults with opioid use disorders in rural Colorado. Substance Abuse Treatment, Prevention, and Policy, 17, 1–11. https://doi.org/10.1186/s13011-021-00424-4
Andersson, H. W., Mosti, M. P., & Nordfjærn, T. (2022). Suicidal ideation among inpatients with substance use disorders: Prevalence, correlates and gender differences. Psychiatry Research, 317, 114848. https://doi.org/10.1016/j.psychres.2022.114848
APA (2022). American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed., text rev.). Washington, D.C.: American Psychiatric Association; 2022. https://doi.org/10.1176/appi.books.9780890425787
Applebaum, A. J., Bullis, J. R., Traeger, L. N., O’Cleirigh, C., Otto, M. W., Pollack, M. H., et al. (2010). Rates of mood and anxiety disorders and contributors to continued heroin use in methadone maintenance patients: A comparison by HIV status. Neurobehavioral HIV Medicine, 49–57. http://dx.doi.org/10.2147/NBHIV.S12371
Archambault, L., Jutras-Aswad, D., Touré, E. H., Artunduaga, A. C., Roy, S., Barbeau, D., et al. (2022). Profiles of patients with opioid use disorders presenting a history of suicidal ideations and attempts. Psychiatric Quarterly, 93(2), 637–650. https://doi.org/10.1007/s11126-022-09978-3
Au, V. Y., Rosic, T., Sanger, N., Hillmer, A., Chawar, C., Worster, A., et al. (2021). Factors associated with opioid overdose during medication-assisted treatment: How can we identify individuals at risk? Harm Reduction Journal, 18, 1–10. https://doi.org/10.1186/s12954-021-00521-4
Barry, D. T., Beitel, M., Cutter, C. J., Garnet, B., Joshi, D., Rosenblum, A., et al. (2011). Exploring relations among traumatic, posttraumatic, and physical pain experiences in methadone-maintained patients. Journal of Pain, 12, 22–28. http://dx.doi.org/10.1016/j.jpain.2010.04.006
Beaumont, S., Magel, T., MacDonald, S., Harrison, S., Schechter, M., & Oviedo-Joekes, E. (2024). Shared decision-making and client-reported dose satisfaction in a longitudinal cohort receiving injectable opioid agonist treatment (iOAT). Substance Abuse Treatment, Prevention, and Policy, 19(1), 1. https://doi.org/10.21203/rs.3.rs-3399610/v1
Becker, W. C., Ganoczy, D., Fiellin, D. A., & Bohnert, A. S. (2015). Buprenorphine/naloxone dose and pain intensity among individuals initiating treatment for opioid use disorder. Journal of Substance Abuse Treatment, 48, 128–131. http://dx.doi.org/10.1016/j.jsat.2014.09.007
Charlson, F., van Ommeren, M., Flaxman, A., Cornett, J., Whiteford, H., & Saxena, S. (2019). New WHO prevalence estimates of mental disorders in conflict settings: A systematic review and meta-analysis. The Lancet, 394(10194), 240–248. https://doi.org/10.1016/s0140-6736(19)30934-1
Dubov, A., Basenko, A., Dymaretskyi, O., & Shoptaw, S. (2024). Impact of the Russian invasion on opioid agonist therapy programs in Ukraine: A qualitative study. Drug and Alcohol Dependence, 255, 111069. https://doi.org/10.1016/j.drugalcdep.2023.111069
Engstrom, M., El-Bassel, N., & Gilbert, L. (2012). Childhood sexual abuse characteristics, intimate partner violence exposure, and psychological distress among women in methadone treatment. Journal of Substance Abuse Treatment, 43, 366–376. http://dx.doi.org/10.1016/j.jsat.2012.01.005
Forkus, S. R., Raudales, A. M., Rafiuddin, H. S., Weiss, N. H., Messman, B. A., & Contractor, A. A. (2023). The Posttraumatic Stress Disorder (PTSD) Checklist for DSM–5: A systematic review of existing psychometric evidence. Clinical Psychology: Science and Practice, 30(1), 110. https://doi.org/10.1037/cps0000111
Hassan, A. N., Bozinoff, N., Jutras-Aswad, D., Socias, M. E., Stewart, S. H., Lim, R., et al. (2023). Patient satisfaction with standard methadone and flexible buprenorphine/naloxone models of care: Results from a pragmatic randomized controlled clinical trial. Journal of Addiction Medicine, 17(1), e49–e56. https://doi.org/10.1097/ADM.0000000000001048
Himelhoch, S., Weber, E., Medoff, D., Charlotte, M., Clayton, S., Wilson, C., et al. (2012). Posttraumatic stress disorder and one-year outcome in methadone maintenance treatment. American Journal on Addictions, 21, 524–530. http://dx.doi.org/10.1111/j.1521-0391.2012.00271.x
Huang, C. L. C., & Lee, C. W. (2013). Factors associated with mortality among heroin users after seeking treatment with methadone: A population-based cohort study in Taiwan. Journal of Substance Abuse Treatment, 44(3), 295–300. https://doi.org/10.1016/j.jsat.2012.08.003
Huhn, A. S., & Dunn, K. E. (2020). Challenges for women entering treatment for opioid use disorder. Current Psychiatry Reports, 22, 1–10. https://doi.org/10.1007/s11920-020-01201-z
Hyland, P., Vallières, F., Shevlin, M., Karatzias, T., Ben-Ezra, M., McElroy, E., et al. (2023). Psychological consequences of war in Ukraine: Assessing changes in mental health among Ukrainian parents. Psychological Medicine, 53(15), 7466–7468. https://doi.org/10.1017/S0033291723000818
Iskandar, S., van Crevel, R., Hidayat, T., Siregar, I. M., Achmad, T. H., van der Ven, A. J., et al. (2013). Severity of psychiatric and physical problems is associated with lower quality of life in methadone patients in Indonesia. American Journal on Addictions, 22(5), 425–431. https://doi.org/10.1111/j.1521-0391.2013.00334.x
Karam, E. G., Salamoun, M. M., Mneimneh, Z. N., Fayyad, J. A., Karam, A. N., Hajjar, R., et al. (2012). War and first onset of suicidality: The role of mental disorders. Psychological Medicine, 42(10), 2109–2118. https://doi.org/10.1017/S0033291712000268
Karatzias, T., Shevlin, M., Ben-Ezra, M., McElroy, E., Redican, E., Vang, M. L., et al. (2023). War exposure, posttraumatic stress disorder, and complex posttraumatic stress disorder among parents living in Ukraine during the Russian war. Acta Psychiatrica Scandinavica, 147(3), 276–285. https://doi.org/10.1111/acps.13529
Klymchuk, V. (2025). Annex to the paper: Prevalence of depression, anxiety, and PTSD symptoms among patients of opioid agonist treatment programmes in Ukraine during wartime. Zenodo. https://doi.org/10.5281/zenodo.15640272
Klymchuk, V., Gorbunova, V., & Ivanchuk, I. (2024). Prevalence of alcohol use, depressive and anxiety symptoms among patients of opioid agonist treatment programmes in Ukraine. Academic Mental Health and Well Being, 1(1). https://doi.org/10.20935/MHealthWellB6210
Kumari, S., Manalai, P., Leong, S., Wooditch, A., Malik, M., & Lawson, W. B. (2016). Factors associated with non-adherence to buprenorphine-naloxone among opioid dependent African-Americans: A retrospective chart review. American Journal on Addictions, 25, 110–117. http://dx.doi.org/10.1111/ajad.12325
Lester, D. (1994). Suicide rates before, during and after the world wars. European Psychiatry, 9(5), 262–264. https://doi.org/10.1017/S092493380000362X
Machavariani, E., Bromberg, D. J., Dumchev, K., Dvoriak, S., Zeziulin, O., Morozova, O., et al. (2023). Design, implementation and preliminary results of a type-2 hybrid cluster-randomized trial of integrating screening and treatment for major depressive disorder into specialty clinics providing opioid agonist therapies in Ukraine. Contemporary Clinical Trials, 131, 107248. https://doi.org/10.1016/j.cct.2023.107248
Madison, C. A., & Eitan, S. (2020). Buprenorphine: Prospective novel therapy for depression and PTSD. Psychological Medicine, 50(6), 881–893. https://doi.org/10.1017/s0033291720000525
Manea, L., Gilbody, S., & McMillan, D. (2012). Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Canadian Medical Association Journal, 184(3), E191–E196. https://doi.org/10.1503/cmaj.110829
Marchand, K. I., Oviedo-Joekes, E., Guh, D., Brissette, S., Marsh, D. C., & Schechter, M. T. (2011). Client satisfaction among participants in a randomized trial comparing oral methadone and injectable diacetylmorphine for long-term opioid-dependency. BMC Health Services Research, 11, 1–10. https://doi.org/10.1186/1472-6963-11-174
McElroy, E., Hyland, P., Shevlin, M., Karatzias, T., Vallières, F., Ben-Ezra, M., et al. (2024). Change in child mental health during the Ukraine war: Evidence from a large sample of parents. European Child & Adolescent Psychiatry, 33(5), 1495–1502. https://doi.org/10.1007/s00787-023-02255-z
Meshberg-Cohen, S., MacLean, R. R., Martin, A. M. S., Sofuoglu, M., & Petrakis, I. L. (2021). Treatment outcomes in individuals diagnosed with comorbid opioid use disorder and posttraumatic stress disorder: A review. Addictive Behaviors, 122, 107026. https://doi.org/10.1016/j.addbeh.2021.107026
Morin, K. A., Eibl, J. K., Gauthier, G., Rush, B., Mushquash, C., Lightfoot, N. E., et al. (2020). A cohort study evaluating the association between concurrent mental disorders, mortality, morbidity, and continuous treatment retention for patients in opioid agonist treatment (OAT) across Ontario, Canada, using administrative health data. Harm Reduction Journal, 17, 1–13. https://doi.org/10.1186/s12954-020-00396-x
Morozova, O., Dvoriak, V., Dumchev, K., Machavariani, E., Bromberg, D. J., Dvoriak, S., et al. (2024). Prevalence and correlates of depression and bipolar disorder among patients maintained on methadone and buprenorphine in Ukraine. International Journal of Mental Health and Addiction, 1–18. https://doi.org/10.1007/s11469-024-01353-6
Naji, L., Rosic, T., Sanger, N., Dennis, B., Worster, A., Paul, J., et al. (2021). The role of cannabis use in suicidal ideation among patients with opioid use disorder. Journal of Addiction Medicine, 15(5), 370–375. https://doi.org/10.1097/adm.0000000000000781
Ngo, H. T., Tait, R. J., & Hulse, G. K. (2011). Hospital psychiatric comorbidity and its role in heroin dependence treatment outcomes using naltrexone implant or methadone maintenance. Journal of Psychopharmacology, 25(6), 774–782. https://doi.org/10.1177/0269881110364266
Padmanathan, P., Forbes, H., Redaniel, M. T., Gunnell, D., Lewer, D., Moran, P., et al. (2022). Self-harm and suicide during and after opioid agonist treatment among primary care patients in England: A cohort study. The Lancet Psychiatry, 9(2), 151–159. https://doi.org/10.1016/s2215-0366(21)00392-8
Pant, S. B., Thapa, S. B., Howard, J., Ojha, S. P., & Lien, L. (2022). Mental disorders and suicidality among opioid agonist treatment service users in Nepal: A cross-sectional study. SSM - Mental Health, 2, 100165. https://doi.org/10.1016/j.ssmmh.2022.100165
Peck, K. R., Moxley-Kelly, N., Badger, G. J., & Sigmon, S. C. (2021). Posttraumatic stress disorder in individuals seeking treatment for opioid use disorder in Vermont. Preventive Medicine, 152, 106817. https://doi.org/10.1016/j.ypmed.2021.106817
Peles, E., Schreiber, S., & Adelson, M. (2006). Factors predicting retention in treatment: 10-year experience of a methadone maintenance treatment (MMT) clinic in Israel. Drug and Alcohol Dependence, 82(3), 211–217. https://doi.org/10.1016/j.drugalcdep.2005.09.004
Preti, A., Demontis, R., Cossu, G., Kalcev, G., Cabras, F., Moro, M. F., et al. (2021). The lifetime prevalence and impact of generalized anxiety disorders in an epidemiologic Italian National Survey carried out by clinicians by means of semi-structured interviews. BMC Psychiatry, 21, 1–8. https://doi.org/10.1186/s12888-021-03042-3
Rathi, P., Joseph, J., Devi, R., & Arya, S. (2024). Assessment of the mental and physical health problems of clients undergoing opioid substitution therapy: A hospital-based cross-sectional study. Annals of Indian Psychiatry, 8(4), 328–331. https://doi.org/10.4103/aip.aip_125_23
Roberts, A. L., Kubzansky, L. D., Chibnik, L. B., Rimm, E. B., & Koenen, K. C. (2020). Association of posttraumatic stress and depressive symptoms with mortality in women. JAMA Network Open, 3(12), e2027935. https://doi.org/10.1001/jamanetworkopen.2020.27935
Roncero, C., Barral, C., Rodríguez-Cintas, L., Pérez-Pazos, J., Martinez-Luna, N., Casas, M., et al. (2016). Psychiatric comorbidities in opioid-dependent patients undergoing a replacement therapy programme in Spain: The PROTEUS study. Psychiatry Research, 243, 174–181. https://doi.org/10.1016/j.psychres.2016.06.024
Rosen, D., Smith, M. L., & Reynolds, C. F. III. (2008). The prevalence of mental and physical health disorders among older methadone patients. American Journal of Geriatric Psychiatry, 16, 488–497. https://doi.org/10.1097/JGP.0b013e31816ff35a
Rosic, T., Au, V. Y., Worster, A., Marsh, D. C., Thabane, L., & Samaan, Z. (2021). Trauma and post-traumatic stress disorder in patients treated for opioid use disorder: Findings from a 12-month cohort study. BJPsych Open, 7(4), e138. https://doi.org/10.1192/bjo.2021.971
Rosic, T., Naji, L., Bawor, M., Dennis, B. B., Plater, C., Marsh, D. C., et al. (2017). The impact of comorbid psychiatric disorders on methadone maintenance treatment in opioid use disorder: A prospective cohort study. Neuropsychiatric Disease and Treatment, 13, 1399–1408. https://doi.org/10.2147/ndt.s129480
Rosic, T., Worster, A., Thabane, L., Marsh, D. C., & Samaan, Z. (2020). Exploring psychological symptoms and associated factors in patients receiving medication-assisted treatment for opioid-use disorder. BJPsych Open, 6(1). https://doi.org/10.1192/bjo.2019.99
Saad, S. N. S., Mohamed, S., Abdullah, N., Ariaratnam, S., & Isa, M. R. (2021). Prevalence of major depressive disorder and its association with erectile dysfunction among clients on methadone maintenance therapy. ASEAN Journal of Psychiatry, 22(4). https://www.aseanjournalofpsychiatry.org/articles/prevalence-of-major-depressive-disorder-and-its-association-with-erectile-dysfunction-among-clients-on-methadone-mainten.pdf
Saraiya, T. C., Helpinstill, S., Gray, D., Hien, D. A., Brady, K. T., Hood, C. O., et al. (2024). The lived experiences and treatment needs of women with opioid use disorder and posttraumatic stress symptoms: A mixed methods study. Journal of Substance Use and Addiction Treatment, 161, 209344. https://doi.org/10.1016/j.josat.2024.209344
Serafini, G., Adavastro, G., Canepa, G., De Berardis, D., Valchera, A., Pompili, M., et al. (2018). The efficacy of buprenorphine in major depression, treatment-resistant depression and suicidal behavior: A systematic review. International Journal of Molecular Sciences, 19(8), 2410. https://doi.org/10.3390/ijms19082410
Smith, J. A., Doidge, M., Hanoa, R., & Frueh, B. C. (2019). A historical examination of military records of US Army suicide, 1819 to 2017. JAMA Network Open, 2(12), e1917448. https://doi.org/10.1001/jamanetworkopen.2019.17
Smoller, J. W. (2016). The genetics of stress-related disorders: PTSD, depression, and anxiety disorders. Neuropsychopharmacology, 41(1), 297–319. https://doi.org/10.1038/npp.2015.266
Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Teoh Bing Fei, J., Yee, A., & Habil, M. H. B. (2016). Psychiatric comorbidity among patients on methadone maintenance therapy and its influence on quality of life. American Journal on Addictions, 25(1), 49–55. https://doi.org/10.1111/ajad.12317
Trafton, J. A., Minkel, J., & Humphreys, K. (2006). Opioid substitution treatment reduces substance use equivalently in patients with and without posttraumatic stress disorder. Journal of Studies on Alcohol, 67, 228–235. http://dx.doi.org/10.15288/jsa.2006.67.228
Villagonzalo, K. A., Dodd, S., Ng, F., Mihaly, S., Langbein, A., & Berk, M. (2011). The relationship between substance use and posttraumatic stress disorder in a methadone maintenance treatment program. Comprehensive Psychiatry, 52, 562–566. http://dx.doi.org/10.1016/j.comppsych.2010.10.001
Vold, J. H., Løberg, E. M., Aas, C. F., Steier, J. A., Johansson, K. A., & Fadnes, L. T. (2022). Prevalence and correlates of suicide attempts in high-risk populations: A cross-sectional study among patients receiving opioid agonist therapy in Norway. BMC Psychiatry, 22(1), 181. https://doi.org/10.1186/s12888-022-03829-y
Wu, L. T., Blazer, D. G., Gersing, K. R., Burchett, B., Swartz, M. S., Mannelli, P., et al. (2013). Comorbid substance use disorders with other Axis I and II mental disorders among treatment-seeking Asian Americans, Native Hawaiians/Pacific Islanders, and mixed-race people. Journal of Psychiatric Research, 47(12), 1940–1948. https://doi.org/10.1016/j.jpsychires.2013.08.022
Zeziulin, O., Mollan, K. R., Shook-Sa, B. E., Hanscom, B., Lancaster, K. E., Dumchev, K., et al. (2021). Depressive symptoms and use of HIV care and medication-assisted treatment among people with HIV who inject drugs. AIDS, 35(3), 495–501. https://doi.org/10.1097/QAD.0000000000002774