Case
Report: Treating Marital Resentment with Radical Honesty in Strategic Family
Therapy {under peer review}
case study
Ezra N. S. Lockhart, Easy Does It Counseling, p.c.;
National University, JFK School of Psychology and Social Sciences, https://orcid.org/0000-0002-4435-9053
Emotionally Focused
Therapy
is commonly treated as treatment-as-usual for entrenched relational resentment
and emotional disconnection, relying on attachment repair through empathic,
emotion-oriented engagement. This case report offers a clinically and ethically
grounded alternative by using Strategic Family Therapy, which emphasizes
therapist-directed systemic pattern disruption rather than intrapsychic
exploration or affective processing. The case involves a heterosexual couple in
their early 40s, married 18 years, presenting with chronic resentment during an
empty-nest transition. Across three 90-minute sessions, the therapist
integrated radical honesty as a directive, systemic intervention with radical
presence as a stabilizing stance. Interventions included direct systemic
confrontation, therapist vulnerability, and strategic reframing, all deployed
within Haley’s strategic model. Data from transcripts, therapist notes, and
patient reflections were examined through thematic, narrative, and content-analytic
methods. Radical honesty, operationalized through explicit therapist-driven
challenge, disrupted ingrained avoidance sequences and generated relational
accountability. Radical presence enabled the therapist to maintain ethical
attunement while sustaining pressure without escalating hostility. The couple
shifted from reciprocal blame to shared responsibility through structured
disruption rather than insight or empathic attunement alone. This case
demonstrates that, within SFT, radical honesty and presence function as
deliberate tools of ethical disruption, supporting relational change where
treatment-as-usual modalities may be insufficient.
Keywords: Marital Therapy, Family Therapy, Truth Disclosure, Psychotherapy,
Time-Limited Psychotherapy, Emotions
Introduction/Background
Couples
therapy addressing entrenched emotional disconnection, such as longstanding
resentment, requires approaches that actively transform relational dynamics to
achieve lasting change (Almeida & Cunha, 2023; Spengler et al., 2024;
Wittenborn et al., 2018). One foundational model that anticipated this systemic
understanding is Jay Haley’s Strategic Family Therapy (SFT; 1973, 1984),
which was among the first to conceptualize the family as a unified system
rather than isolated individuals. Rooted in systems theory (Broderick, 1993)
and influenced by Gregory Bateson’s communication theory (Bateson, 1972) and
Milton Erickson’s hypnotherapy (Haley, 1958, 1959, 1993), Haley developed a
directive, goal-oriented approach emphasizing therapist authority, power, and
systemic realignment. His early work also addressed the ethical implications of
therapist influence and consent within hypnosis (Haley & Erickson, 1959).
This approach marked a foundational shift from intrapsychic focus to relational
dynamics, viewing symptoms as strategic behaviors embedded in relational
networks rather than isolated issues (Haley, 1967, 1973; [Author], 2025a;
Villa, 2024). Minuchin (2007) recognized Haley’s influence as foundational to
modern family therapy.
In
addition to its clinical impact, Haley’s work carries a vital ethical
dimension. Recent scholarship situates his approach within a bioethical
framework emphasizing relational accountability, clinical responsibility, and
ethical governance of therapeutic influence (American Association of Marriage
and Family Therapy [AAMFT], 2015; [Author], 2025a). Haley challenged
traditional notions of therapist neutrality and patient autonomy by promoting
ethically grounded, goal-oriented interventions that balance agency with
beneficence and justice within relational systems. This perspective deepens
understanding of Haley’s methods as ethically responsible strategic practice,
especially amid critiques that paradoxical techniques have been viewed as
manipulative or controlling (e.g., critics in Anderson & Erstling, 1983;
Solovey & Duncan, 1992; Wilner et al., 1988)
Within
this modernist strategic tradition, this study examines how Haley–informed
strategic interventions operate to confront avoidance, foster accountability,
and support restoration of authentic emotional connection in brief couples
therapy. Radical honesty, while not a formal Haley technique, is explored here
as a clinically grounded and theoretically compatible intervention defined as
direct systemic confrontation integrated with relational mindfulness and
radical presence (Lord, 2017; McNamee, 2016, 2020, 2021; Morales, 2020;
Shotter, 2005). This study articulates how radical honesty functions as an
embedded principle within Haley’s framework through therapist presence,
systemic intervention, and ethically grounded confrontation. Given the inherent
risk of shame in radical honesty, its ethical viability depends on sensitive
therapist attunement and supportive relational context (Williams, 2017).
Through in-depth case analysis, it contributes to early empirical groundwork by
evaluating radical honesty’s clinical utility, theoretical coherence, and
ethical viability.
This
qualitative single-case study analyzes session transcripts, therapist process
notes, and reflections using thematic, narrative, and content methodologies to
capture emotional and interactional shifts (Braun & Clarke, 2006;
Krippendorff, 2018). Triangulating multiple data sources enhances analytic
depth and supports clinical validity, clarifying how strategic therapist
engagement disrupts rigid cycles of resentment and promotes authentic intimacy
(Donkoh & Mensah, 2023). Meta-analytic evidence broadly supports the
effectiveness of couple therapy across designs and timeframes, providing a
general empirical foundation for focused strategic interventions (Roddy et al.,
2020). Methodological rigor is emphasized not simply as procedural detail but
as integral to the study’s epistemological orientation and ethical commitment
to responsible knowledge production.
By
elucidating the therapist’s active and ethically engaged role in catalyzing
systemic realignment through radical honesty, the study contributes to
contemporary discourse on strategic family therapy and relational mindfulness.
It demonstrates that lasting relational restoration depends on the therapist’s
capacity to engage difficult truths with clarity, intention, and ethical
responsibility. These core elements reflect and extend Haley’s enduring legacy
in modern clinical practice.
Theoretical Foundation
This study is
grounded in a systemic theoretical framework that conceptualizes resentment as
a relationally co-constructed pattern, rather than an isolated intrapsychic
emotion. Rooted in systems theory, resentment is understood to emerge from
recursive cycles of avoidance, defensiveness, and blame (Bateson, 1972;
Broderick, 1993; Haley, 1973, 1984; Villa, 2024). These entrenched
interactional patterns maintain emotional distance and relational gridlock over
time. Within this view, effective intervention requires not merely insight or
empathy, but strategic disruption—deliberate therapeutic actions that shift
rigid relational dynamics and generate new patterns of engagement (Haley,
1984).
SFT, as developed by
Jay Haley, provides the clinical foundation for this approach. Haley’s model
emphasizes directive, pragmatic interventions that target the structural and
communicative aspects of dysfunctional relationships. However, Haley's contributions
extend beyond methodology. [Author]’s (2025a) ethical reappraisal of Haley’s
work foregrounds the bioethical foundations of SFT and traces their
codification in the AAMFT Code of Ethics, institutionalizing their relevance
across systemic models of practice.
Within
this ethically anchored framework, the therapist assumes a dual role: not only
as a strategist, but also as a morally accountable change agent, responsible
for both the clinical and ethical impact of therapeutic interventions
([Author], 2025b). This perspective is further elaborated in [Author]’s (2025b)
clinical exegesis of Strategies of Psychotherapy, which elucidates
symptoms as communicative behaviors embedded in relational systems. [Author]’s
synthesis of Haley’s methods with contemporary bioethics deepens the ethical
accountability of systemic interventions while preserving their pragmatic
focus.
Complementing
this strategic orientation is the concept of radical presence, drawn from
Shotter’s (2005) theory of expressive-responsive dialogue, itself rooted in
Wittgensteinian language games (Harris, 1990; Hintikka, 1979). Expanded by
McNamee (2016), radical presence positions the therapist as an emotionally
attuned, dialogically responsive participant who grounds their interventions in
emotional honesty and relational co-construction. Far from opposing strategic
direction, radical presence enhances it: by softening resistance and building
trust, it makes directive interventions more receivable and impactful. Radical
presence, rooted in Bateson’s (1972) systemic epistemology, acts as both a
relational stance and a moral posture, aligning with the ethical commitments
articulated in [Author]’s reinterpretation of Haley.
Together,
strategic pragmatism, ethical accountability, and dialogical presence form the
theoretical foundation of this study. They support an approach that aims to
disrupt entrenched relational patterns while attending to the emotional,
ethical, and systemic complexity of couples therapy.
Research Design and Methodology
This
study employed a structured qualitative single-case design to investigate the
impact of strategic interventions, particularly radical honesty and emotional
vulnerability, on entrenched relational dynamics in a couple experiencing
longstanding resentment and emotional disconnection (Carlonet al., 2012; Stake,
1995, 2013). Prioritizing process over outcome, the design aligned with
systemic epistemology and psychotherapy case study conventions (Bruner, 1990;
McLeod, 2011).
Application of Study
Design
This
clinical case report adheres to the CARE (CAse REport) guidelines (Gagnier et
al., 2013) to ensure clarity, transparency, and reproducibility in clinical
case documentation. Given the psychotherapy context, the report is further
informed by psychotherapy-specific standards from Eells (2022) and the Case
Study Evaluation-tool (CaSE) framework (Kaluzeviciute, 2021), which emphasize
thorough clinical formulation, analytic rigor, and contextualized
interpretation. Together, these frameworks guided the structured presentation
of clinical data and analytic methods, supporting ethical, systematic, and
practice-relevant case reporting.
Participants and Setting
The
case involved a heterosexual couple presenting with longstanding emotional
estrangement and escalating resentment. The intervention was conducted in
Louisiana, United States, in November 2024 within an outpatient clinical
setting. Services were delivered in compliance with regulatory requirements. Clinical
intake revealed entrenched avoidance, emotional defensiveness, and chronic
dissatisfaction. A brief therapy format consisting of three 90-minute sessions
was used. Detailed contextual information about each partner and their
relational history was collected to inform the intervention and interpret
interactional patterns (Roddy et al., 2020).
Therapist Reflexivity
Therapist
reflexivity was a foundational component of this investigation. The clinician
also served as the principal investigator, necessitating careful navigation of
dual roles. Reflexive strategies included: (a) immediate post-session
journaling, (b) peer consultation, and (c) a comprehensive audit trail. These
practices aimed to identify bias, enhance analytic transparency, and refine
clinical responsiveness (Bolton, 2010; Finlay, 2002).
Case Reporting
The
study also integrated the CARE (CAse REport) guidelines for psychotherapy case
reporting (Gagnier et al., 2013), psychotherapy-specific standards (Eells,
2022), and the CaSE (Case Study Evaluation-tool) framework (Kaluzeviciute,
2021), ensuring ethical rigor and clarity.
Therapeutic Orientation and Case Formulation
The
intervention followed the principles of SFT, emphasizing pattern disruption,
directive interventions, and recursive systemic analysis (Haley, 1973, 1984).
Within the first 15–20 minutes of the initial session, the therapist formulated
a working hypothesis focused on the couple’s interactional cycles rather than
the surface-level presenting problem (e.g., job instability). The conceptual
framework drew from [Author]’s (2025a, 2025b) ethical reinterpretation of SFT,
where the therapist is framed as a morally accountable change agent, rather
than a neutral operator of techniques. The therapist's stance integrated
strategic planning with radical presence–defined as real-time emotional
attunement, non-defensiveness, and dialogical responsiveness (Lord, 2017;
McNamee, 2021; Morales, 2020; Shotter, 2005).
Therapeutic Stance
Relational
mindfulness served as a guiding therapeutic stance. It emphasized:
●
Present-centered
awareness of emotional and interpersonal dynamics
●
Embodied
attunement to interactional shifts
●
Moral
responsiveness to patient vulnerabilities
This approach supports the delivery
of directive interventions with both strategic precision and ethical
sensitivity (Lord, 2017; McNamee, 2021).
Treatment Principles
Drawing
from SFT and supported by the concept of radical presence, the intervention
employed four core treatment principles. These principles guided moment-to-moment therapeutic
decision-making and served as the clinical scaffolding for the case:
·
Radical
Truth-Telling. Partners were encouraged to speak with directness and emotional
clarity, surfacing long-suppressed resentments and unmet needs. This principle
aimed to disrupt collusive silences and emotional avoidance (McNamee, 2016;
Williams, 2017).
·
Patient
Action Over Comfort. The couple was asked to take emotionally challenging
steps toward reconnection even when doing so elicited discomfort. This
principle follows Haley’s directive logic: change occurs through strategic
behavioral shifts, not emotional ease (Haley, 1984; McNamee, 2020).
·
Challenging
Defensive Patterns. The therapist directly confronted recursive patterns of blame,
emotional withdraw, stonewalling, and minimization. Interventions were designed
to expose and interrupt these defenses to enable more vulnerable engagement
(Haley, 1984; McNamee, 2021).
·
Emotional
Vulnerability. The therapist’s radical presence modeled relational risk-taking
and emotional openness. This stance invited both partners to move beyond
entrenched roles and toward deeper relational repair (Shotter, 2005; McNamee,
2016).
These
principles operated together within a time-limited, strategic format that
emphasized pragmatic change over emotional catharsis, aligning with the
modernist-pragmatist ethos of SFT.
Data Collection
Multiple
data sources were triangulated to
ensure validity and depth:
●
Verbatim
session transcripts captured the interactional flow and emotional tone of
therapy.
●
Therapist
process notes written immediately after each session, documenting impressions,
hypotheses, and clinical decisions.
●
Patient
reflections collected over the phone via structured prompts after the couple
returned home following each session to elicit clients’ perceived impact of
interventions.
These
sources offered a layered,
process-rich understanding of therapeutic change (Roddy et al., 2020).
Data Processing and
Coding Workflow
Data
analysis followed a multi-stage,
technology-supported, offline workflow:
●
Manual
thematic coding in NVivo software
●
Automated
coding using a custom Python pipeline with spaCy and pandas libraries
for:
○
Named
entity recognition
○
Pattern
detection
○
Lexical
comparison across datasets
This
dual offline system ensured human interpretive depth, computational
consistency, and data security and privacy (Jockers & Thalken, 2020;
Khandekar et al., 2021). Outputs were cross-referenced and validated through
peer consultation and iterative raw data review. Figure 1 presents the
qualitative coding and validation pipeline.
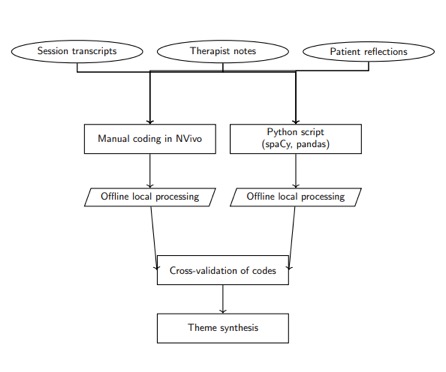
Figure 1. Qualitative
Coding and Cross-Validation Workflow
Analytic Strategy
Three qualitative methodologies were independently
applied to the validated codes:
Table 1. Analytic Strategy
|
Method
|
Purpose
|
|
Thematic Analysis
|
Identify recurring emotional
and interactional patterns (Braun & Clarke, 2006)
|
|
Content Analysis
|
Track discourse structure and
shifts pre/post intervention (Krippendorff, 2018)
|
|
Narrative Analysis
|
Interpret evolving self-narratives and
relational storylines (Angus & McLeod, 2004)
|
Converging
findings from these approaches allowed triangulation and enhanced interpretive
credibility. When analytic contradictions arose, they were systematically
resolved through reflexive journaling and return to primary data.
Operationalization of Constructs and Principles
Table 2 details how key therapeutic
constructs and treatment principles were operationalized within the clinical
case study, providing observable indicators for each.
Table 2. Constructs and Principles
Operationalization
|
Construct / Principle
|
Definition
|
Operational
Indicators
|
Data Source(s)
|
|
Resentment
|
Accumulated emotional injury from unresolved
grievances
|
Blame statements, repetitive complaint cycles,
historical references to unmet needs
|
Session transcripts, patient reflections
|
|
Emotional Defensiveness
|
Reactive protection of self from perceived
emotional threat
|
Deflection, justification, denial,
stonewalling
|
Therapist notes, transcript dialogue
|
|
Relational Disconnection
|
Chronic absence of intimacy and empathic
responsiveness
|
Monologic speech, low affect, absence of eye
contact, narrative distancing
|
Session observations, therapist process notes
|
|
Radical Truth-Telling
|
Honest expression of difficult emotions and
truths
|
Use of emotionally direct language,
confrontation of avoided topics
|
Session transcripts, therapist coding
|
|
Patient Action Over Comfort
|
Behavior that prioritizes growth over
immediate emotional relief
|
Willingness to remain in conflictual dialogue,
acceptance of discomfort for long-term change
|
Post-session reflections, in-session behavior
|
|
Challenging Defensive Patterns
|
Direct therapeutic interventions targeting
avoidance or blame
|
Therapist confrontation of defenses, partner
response to these challenges
|
Process notes, session transcripts
|
|
Emotional Vulnerability
|
Expression of core emotions that invite
intimacy and connection
|
Tearfulness, expressions of fear or shame,
emotional risk-taking
|
Verbatim dialogue, therapist observation
|
Note.
Constructs
were defined a priori based on theoretical literature, then iteratively
refined through reflexive coding and peer consultation. Operational indicators
refer to observable or reportable behaviors used to infer each construct’s
presence or emergence. Data sources include triangulated qualitative materials
(session transcripts, therapist notes, patient reflections) analyzed using
thematic, content, and narrative methods. A codebook was developed.
Theoretical
Distinctions and Methodological Clarifications
Although resentment in couples
is often conceptualized as an attachment injury rooted in emotional
disconnection (Almeida & Cunha, 2023; Spengler et al., 2024; Wittenborn et
al., 2018), this study adopts a different framework. Emotionally Focused
Therapy (EFT), supported by decades of research (Johnson & Greenberg, 1985,
1987), has shown consistent benefits in enhancing relationship satisfaction and
emotional bonding. A recent randomized controlled trial found that couples
receiving EFT reported greater improvements in relationship quality and
reductions in depressive symptoms compared to those receiving
treatment-as-usual (Wittenborn et al., 2018; Spengler et al., 2024).
Despite
its empirical support and theoretical coherence with emotion-focused models,
this study situates resentment within a strategic, systemic paradigm grounded
in SFT. This approach prioritizes interactional pattern disruption and
pragmatic intervention (Bobrow & Ray, 2005; [Author], 2025d) over affective
transformation through empathy and attachment repair (Angus & Greenberg,
2011; Johnson, 2004). These frameworks differ epistemologically. EFT is rooted
in humanistic, emotion-centered traditions, whereas SFT aligns with
action-oriented pragmatism. Drawing from Socratic refutation and Deweyan logic,
SFT casts the therapist as a disruptor of rigid relational patterns to catalyze
behavioral and cognitive shifts ([Author], 2025c). Emotional expression is functional
rather than foundational, serving strategic ends. Radical presence,
conceptualized by Shotter (2005) and expanded by McNamee (2016), supports this
by grounding the therapist in dialogical sincerity while preserving directive
authority. Techniques that invite authentic emotional expression (Brothers,
1993; Daneshpour, 2024; Villa, 2024) are used not to replace but to enhance the impact of
Haley’s ethically accountable interventions ([Author], 2024).
Methodological
Limitations
This
study operates within a systemic epistemology that challenges linear and
symptom-focused models of change. Within this tradition:
●
Andersen
(1991) advocates entering therapeutic dialogue without preformulated
hypotheses, enabling the emergence of the not-yet-seen and not-yet-thought-of.
●
Solution-focused
brief therapy privileges generative solution talk over problem talk (de Shazer,
1985, 1988; de Shazer & Berg, 1997).
●
Narrative
therapy seeks to externalize dominant problem narratives and open alternative
storylines (Roth & Epston, 1998; White & Epston, 1990).
●
Milan
systemic approaches foreground recursive relational dynamics as clinically
salient, often more so than any single symptom (Brown, 2012).
Collectively,
these traditions underscore systemic therapy’s commitment to decentering the
initially defined problem and prioritizing relational and contextual
complexity.
Conventional
pre- and post-treatment measures risk oversimplifying the recursive,
co-constructed processes that systemic therapy aims to explore (Carr, 2019;
Vetere & Stratton, 2016). In line with this orientation, the study did not
use formal psychometric tools, opting instead for process notes, transcript
analysis, and patient reflections to track progress (Asen, 2002). This reflects
a deliberate methodological stance: standardized metrics may not capture the
situated, relational nature of systemic change (Hedges, 2005; McNamee &
Gergen, 2004).
Implications
While
this process-oriented approach yields rich contextual insight, it lacks:
●
Objective
benchmarking with standardized outcome measures
●
Quantitative
generalizability across populations or studies
●
Empirical
calibration using established reliability metrics
Systemic
therapy’s emphasis on meaning, dialogue, and context can conflict with
reductionist measurement tools. Nonetheless, the study demonstrates that
rigorous reflexivity and triangulated analysis can provide valid insight into
relational change even without numerical outcomes.
Recommendations for Future Research
Table 2. Future
Research Recommendations
|
Recommendation
|
Purpose
|
|
Mixed-Methods Integration
|
Blend qualitative insights with pre/post
quantitative tools (e.g., ECR, DAS)
|
|
Longitudinal Follow-Up
|
Track whether change processes are durable
beyond the therapy window
|
|
Observer-Based Process
Ratings
|
Include third-party coding of sessions (e.g.,
SASB, CIRS) for independent validation
|
|
Dual Accountability Models
|
Combine systemic interpretive methods with
replicable outcome metrics to bridge paradigmatic gaps
|
Future
research could adopt these strategies without abandoning systemic epistemology.
Rather than replace interpretive depth, standardized metrics may complement it.
This might invigorate methodological rigor in systemic research and facilitate
cross-paradigm integration in broader couple and family therapy scholarship.
Clinical
Case Report
This
case report describes a heterosexual couple in their early 40s presenting with
entrenched emotional disconnection and chronic resentment, persisting over a
decade. Both partners reported mutual feelings of abandonment and communication
breakdown, exacerbated during their recent empty-nest transition. Early
relational neglect, emotional avoidance, and unresolved conflict characterized
the dynamic.
Patient Information
The
couple consisted of a 42-year-old female executive in a technology firm
(Partner 1) and a 45-year-old male construction worker (Partner 2). They had
been married for 18 years and were in the early stages of an empty-nest
transition after raising two children. Both partners identified significant emotional distance
and longstanding resentment as central issues in their relationship.
Partner
1 was raised in a family environment that discouraged emotional expression,
shaping her reliance on control, logic, and emotional suppression as protective
strategies. In the marital relationship, she frequently withdrew from conflict,
driven by a deep-seated fear of rejection and abandonment. She reported
struggling to express vulnerability, often masking emotional pain to avoid
perceived harm or misinterpretation.
Partner
2 was similarly raised in an emotionally distant household where
self-sufficiency was emphasized and vulnerability was discouraged. His typical
coping strategy involved withdrawal and emotional avoidance, especially when
confronted with his partner’s emotional needs. He described feeling overwhelmed
and inadequate in emotionally charged situations, leading to further
disengagement.
The
relationship’s emotional trajectory shifted following the birth of their second
child. Early in their marriage, the couple described periods of intimacy and
connection; however, as parenting demands increased and careers progressed, the
emotional bond between them weakened. Financial pressures, unresolved family
crises, and unmet emotional needs further deepened the relational divide.
Although both partners expressed a desire to reconnect, they felt uncertain
about how to move beyond the entrenched resentment and restore intimacy.
Therapist Information
The
therapist is both investigator and clinician, embodying the role of a strategic
systemic change agent deeply informed by intersectional identities: Black,
Indigenous, and Person of Color (BIPOC) and Asian American, Native Hawaiian,
and Pacific Islander (AANHPI), male-bodied, neurodiverse, LGBTQIA+. Drawing on
[Author]’s (2025a; 2025b) ethical reappraisal of Haley’s SFT, therapeutic work
is framed not merely as intervention delivery but as an ethically accountable
process integrating bioethical principles of nonmaleficence, beneficence, and
relational justice. The therapist’s role includes strategically disrupting
entrenched relational patterns while modeling emotional vulnerability and
relational mindfulness, fostering radical truth-telling and patient action over
comfort.
Radical
presence (Shotter, 2005; McNamee, 2016) is enacted as a core clinical stance
characterized by moment-by-moment attunement, emotional honesty, and dialogical
engagement. This grounding enabled the therapist to dynamically respond to
patient defenses and promote genuine emotional expression. The therapeutic
relationship functioned as both a mirror and an experiential model for the
couple’s growing capacity for emotional engagement and vulnerability (Zhu,
2018).
Reflective
practices shaped clinical decisions throughout the brief therapy. For example,
therapist journaling after Session 1 revealed subtle patient resistance to
confrontation, leading to modifications of
intervention tone and pacing in subsequent sessions. Relational mindfulness was
demonstrated during moments of emotional withdrawal when the therapist
maintained presence and attunement through intentional silence and empathetic
gestures in Session 2, enabling the couple to safely process difficult emotions
together.
Clinical Findings
The
couple presented with longstanding relational difficulties characterized by
emotional distance, resentment, and avoidance of vulnerability. Early in
therapy, both partners demonstrated defensiveness and hesitancy to engage in
open communication. One partner expressed, “I don’t... I mean, I don’t know
how to just say it. I don’t want to hurt him, but I can’t pretend everything is
fine either” (Partner 1, session 1), illustrating the difficulty in
articulating painful emotions. The other partner shared, “I’ve been avoiding
you, not because I don’t love you, but because I’m afraid if I try to open up,
it will just make things worse” (Partner 2, session 3), highlighting fear
of vulnerability as a core issue.
Observations
revealed a pattern of emotional withdrawal and mutual blame, with resentment
functioning as a shield against deeper emotional exposure. The couple’s
communication was marked by avoidance and defensiveness, which reinforced their
relational gridlock. The therapist noted early resistance to radical honesty
interventions, as seen in the partner’s hesitations, and emphasized the need
for confronting uncomfortable truths to facilitate change: “You believe you
are here to heal. But are you ready for what healing really requires? Healing
is not about softening the blow or wrapping it in a comfortable blanket”
(Therapist, session 1).
Despite
initial discomfort, the couple gradually began to articulate emotions more
openly, recognizing their individual contributions to the relational
dysfunction. The clinical presentation was consistent with entrenched patterns
of emotional avoidance and a lack of mutual accountability, which had become
barriers to intimacy and effective communication.
Timeline
Table 3
outlines the key clinical events, intervention strategies, and therapeutic
milestones across the three-session treatment timeline. In alignment with
Haley’s (1984) SFT, as expanded by [Author] (2025c), each session was
structured around deliberately sequenced interventions aimed at disrupting
entrenched relational patterns and catalyzing systemic change. The table
details the session-by-session application of strategic, paradoxical, and
performance-based techniques, patient responses, and the rationale for each
intervention. This structured progression reflects SFT’s commitment to
pragmatic, action-oriented change grounded in systems theory and strategic
epistemology ([Author], 2025c; Watzlawick et al., 1974).
Table 3. Strategic
Therapy Process: Timeline, Interventions, and Shifts
|
Session / Week
|
Therapeutic Focus
|
Intervention(s)
|
Observed Patient
Shifts
|
Strategic Rationale /
Purpose
|
|
1
|
Initial pattern mapping; disrupt emotional
avoidance
|
Strategic Confrontation: Directly challenged
blame dynamics
Reframing: Resentment as
self-protection
|
Patients showed resistance but began
acknowledging internal distress; emotional defensiveness surfaced quickly
|
Expose recursive blame patterns; provoke
discomfort to stimulate system destabilization
|
|
Radical Presence (Therapist): Moment-to-moment
attunement with challenge
|
Partner 1 expressed fear of vulnerability;
Partner 2 admitted fear of escalation
|
Set foundation for safe but confronting
environment
|
|
2
|
Escalate emotional risk-taking; disrupt mutual
avoidance loop
|
Prescribing the Symptom (in reverse):
Invited couple to avoid each other completely for a day
|
Partner 2 reported emotional discomfort;
Partner 1 described internal tension and longing for reconnection
|
Highlight futility of avoidance; provoke
systemic insight through experiential contradiction
|
|
Double Bind: “You can stay
silent, but silence speaks too. Either way, you are choosing your message.”
|
Couple began to articulate unspoken
expectations and repressed anger
|
Undermine passive roles and introduce
conscious choice into unconscious patterns
|
|
Strategic Questioning: “What are you
getting from avoiding responsibility?”
|
Insight into their co-maintained gridlock;
defensiveness reduced
|
Evoke cognitive dissonance to challenge
habitual narratives
|
|
3
|
Consolidation of
accountability; establish forward motion
|
Guided Ordeal: Structured
vulnerability exercise (disclosure of "most withheld truth")
|
Both partners expressed raw emotional truths
without defensive rupture
|
Deepen engagement through emotional risk and
relational exposure
|
|
Role Repositioning: Partner 2 asked to
take temporary lead in emotional expression
|
Shift in relational balance
observed; Partner 2 showed increased agency
|
Reconfigure emotional labor; test new
interactional roles
|
|
Therapist-as-Problem (light form):
Therapist adopted intentionally ambivalent stance on "progress"
|
Couple began validating each
other rather than relying on therapist affirmation
|
Push dyadic responsibility; reduce
triangulation
|
Note.
Interventions
in Strategic Family Therapy are not pre‑scheduled techniques
but strategically selected maneuvers enacted in response to interactional dynamics observed in session.
This table reflects the emergent structure of the therapeutic process.
Diagnostic Assessment
In
line with the CARE reporting standards, diagnostic considerations were
addressed prior to intervention. No formal DSM‑5 or ICD‑10 psychiatric
diagnoses were assigned to either partner, as the presenting difficulties were relational in
nature and consistent with entrenched systemic patterns rather than individual
psychopathology. Both partners exhibited chronic avoidance of vulnerability,
emotional defensiveness, and persistent resentment rooted in longstanding relational
dynamics. These interactional processes were conceptualized within a systemic
framework, consistent with SFT.
No
laboratory, imaging, or psychometric instruments were administered, as the
therapeutic focus was on dyadic interactional change rather than individual
symptom measurement. Differential diagnostic considerations, such as mood or
anxiety disorders, were explored through clinical interview but ruled out as
primary drivers of the presenting problem; the evidence suggested that the
symptoms were best explained by relational avoidance and recursive blame
dynamics rather than a discrete psychiatric condition. Prognostic expectations
were therefore tied to the couple’s capacity for sustained relational change
through strategic systemic intervention.
Case Formulation and
Conceptualization
Upon
meeting the couple in their initial session, I was able to conceptualize their
case within the first 15 to 20 minutes based on their interactions, body
language, and emotional distance. Within this brief window, I identified the
core issues: resentment, emotional defensiveness, and a clear avoidance of
vulnerability. These emotional dynamics were not merely reactive to isolated
events but reflected longstanding relational patterns. The couple had become
entrenched in a cycle in which each partner’s emotional withdrawal and unspoken
resentments prevented meaningful communication and connection.
SFT is
designed to be brief, and this approach was fitting for the couple’s needs. SFT
does not focus on individual psychopathology and instead focuses on recursive
interactional patterns. Therefore, I quickly assessed that their relational
gridlock was rooted in avoidance and emotional disconnection, not surface-level
disputes. The couple was stuck in a defensive stance, where emotional openness
was equated with risk of rejection, escalation, or failure. Over time, this
avoidance created increasing emotional distance. The therapeutic goal,
therefore, was to rapidly disrupt this cycle.
It
became evident early in treatment that the couple was caught in a closed
feedback loop of emotional avoidance, defensiveness, and mutual blame. Each
partner reinforced the very dynamics they sought to escape. These patterns had
hardened into an entrenched system of emotional standoff, sustained by fear,
pride, and self-protection.
Partner
1’s emotional withdrawal and controlling tendencies were conceptualized as
adaptive responses shaped by family norms that discouraged emotional
expression. Her tendency to intellectualize and retreat during conflict had
become a mechanism to avoid perceived chaos and vulnerability. This was evident
in her own words:
"I
don’t... I mean, I don’t know how to just say it. I don’t want to hurt him, but
I can’t pretend everything is fine either." (Partner 1, session 1)
Partner
2’s avoidance of emotional engagement, in contrast, was driven by an implicit
fear of escalation and rejection. His internalized belief that vulnerability
equates to weakness likely stemmed from early familial experiences where
emotion was either punished or ignored. He expressed this directly in the final
session:
"I’ve
been avoiding you, not because I don’t love you, but because I’m afraid if I
try to open up, it will just make things worse." (Partner 2, session 3)
The
couple’s emotional gridlock functioned as a systemic communicative loop driven
by avoidance and reciprocal blame, with resentment serving both as a symptom of
their distress and a defensive strategy to avoid confronting painful truths.
The therapist’s strategic focus was on disrupting this loop by fostering
radical honesty, emotional risk-taking, and personal accountability,
cultivating a therapeutic space that emphasized tolerance for discomfort and
confrontation over premature comfort. As framed in one of the early
confrontations:
"Resentment
is an easy excuse... It is your decision to keep holding onto it, even as it
destroys you both. Do you have the courage to stop pretending that the other
person is the cause of your suffering?" (Therapist, session 2)
This
strategic confrontation reframed their emotional pain as co-constructed and
maintained, rather than externally inflicted. By emphasizing personal accountability over blame,
the intervention pushed the partners to acknowledge their complicity in the
dynamic. Throughout the work, I emphasized that emotional risk not premature
comfort was essential. Offering soothing reassurance in early sessions would
have only reinforced their avoidant strategies. Instead, I guided them to face
the discomfort of truth-telling and relational exposure as necessary steps
toward intimacy and repair. As posed in session one:
"The
only thing you can change here is not the other, but you... Do you have the
guts to see the selfishness, the fear, the insecurity that has led you to act
in ways that are not entirely innocent, not entirely pure?" (Therapist, session 1)
By
confronting these uncomfortable truths, the couple began to access deeper
emotional layers that had been buried beneath protective behaviors. The
formulation and therapeutic strategy worked in tandem: to expose, destabilize,
and then reorient the couple toward a new mode of relating that allowed for
genuine connection grounded in emotional honesty and mutual responsibility.
Therapeutic Intervention
While
Table 1 illustrates the sequence of interventions across three sessions, these
were not predetermined steps in a manualized protocol. In alignment with SFT,
the intervention strategy unfolded as a function of the therapist’s expertise,
reflexivity, and in‑the‑moment assessment of the couple’s interactional
patterns. Thus, the ‘protocol’ is best understood as a structured decision‑making process
responsive to systemic dynamics, rather than a rigid, pre‑planned session
outline.
The
therapy began with interventions designed to disrupt the couple’s entrenched
patterns of avoidance, defensiveness, and mutual resentment, and promote
emotional honesty. These interactional cycles were understood as recursive
systemic loops maintaining emotional disconnection and relational gridlock
(Haley, 1984; Villa, 2024). From the outset, interventions were enacted within the
therapist’s radical presence via a dialogical stance emphasizing
moment-to-moment emotional honesty, attunement, and ethical accountability
(McNamee, 2016; Shotter, 2005). This stance fostered a relational climate in
which vulnerability and directness could be both invited and tolerated,
allowing for strategic disruption of defensive patterns.
Early in
therapy, radical truth-telling was enacted as a core principle to challenge the
couple’s avoidance and encourage the candid expression of long-suppressed
resentments:
"You
sit here, with resentment between you. It is not a soft resentment, no—this is
the kind of thing that gnaws at your soul... You don’t need sympathy. You need
to confront the rawness of your own lives—of your own choices." (Therapist, session
1)
This
confrontation was designed to break through the couple’s habitual use of
resentment as a defensive identity and avoidance strategy, in line with the
principle of challenging defensive patterns (Haley, 1984; McNamee, 2021). The
therapist emphasized that healing required patient action over comfort,
encouraging the partners to face painful truths rather than seek emotional
relief:
"Healing
is not about softening the blow or wrapping it in a comfortable blanket...
There is only facing the truth." (Therapist, session 1)
To
further shift the systemic interaction, the therapist highlighted the necessity
of personal accountability and interrupting blame cycles:
"Resentment
is an easy excuse... Do you have the courage to stop pretending that the other
person is the cause of your suffering?" (Therapist, session 2)
"The
only thing you can change here is not the other, but you... Do you have the
guts to see the selfishness, the fear, the insecurity that has led you to act
in ways that are not entirely innocent?" (Therapist, session 1)
These
interventions operationalized the therapist’s role as an ethical change agent,
not merely an observer, as emphasized in [Author]’s (2025a, 2025b) ethical
reappraisal of SFT. The therapist strategically guided the couple toward
rupturing maladaptive interactional loops, fostering a relational space where
responsibility and vulnerability could co-exist in a controlled environment
with the risk of harm (Haley, 1984; Villa, 2024).
The
therapeutic relationship itself functioned as a site of intervention, modeled
through radical presence and emotional vulnerability (McNamee, 2016; Shotter,
2005). The therapist invited the couple to inhabit discomfort and uncertainty:
"You
may not have the answers right now... Can you face each other, with all your
pain and your anger, and see each other clearly?" (Therapist, session 2)
As
therapy progressed, the therapist further challenged the couple to confront the
consequences of their patterns and choose active change:
"So
what comes next is not healing, not in the way that you want it... The choice
is yours. But no one is coming to save you." (Therapist, session 3)
The work
culminated in an exercise of radical vulnerability, encouraging the partners to
reveal moments of failure and imperfection without expectation of immediate
forgiveness; and, thus, disrupting habitual defenses and paving the way for
authentic connection:
"This
is your moment to act—not out of some moral duty, but out of a deep sense of
freedom that comes from finally understanding you are free to choose
differently." (Therapist, session 3)
Through
the consistent enactment of these strategic interventions within a relationally
attuned and ethically grounded framework, the couple began to interrupt their
dysfunctional relational cycles and move toward new patterns of emotional
honesty and accountability.
Beyond disrupting
dysfunctional relational patterns and promoting second-order change, specific
strategies cultivated radical honesty and vulnerability. The couple engaged in
structured truth-telling exercises designed to surface previously avoided emotions.
For instance, in Session 3, each partner was invited to share a “most withheld
truth” about their feelings, guarded fears, or resentments, creating a space
for raw emotional disclosure.
Strategic enactments
also included role reassignments aimed at shifting relational hierarchies and
encouraging new patterns of interaction. The therapist invited Partner 2 to
take a leading role in expressing emotions, challenging traditional emotional distancing,
and reconfiguring the couple’s interactional roles. These actions sought to
destabilize entrenched patterns of blame and avoidance, fostering opportunities
for repair and intimacy aligned with SFT principles.
Follow-up and Outcomes
By the
conclusion of therapy, the couple demonstrated significant progress in
interrupting their previously entrenched systemic patterns of avoidance,
defensiveness, and resentment. Initially marked by emotional distance and a
lack of authentic communication, the partners developed an increased capacity
for radical honesty and emotional vulnerability. This shift reflected a gradual
reconfiguration of their interactional patterns within the therapeutic system.
One of
the most salient outcomes was the couple’s enhanced ability to articulate their
emotions and engage in difficult conversations without resorting to avoidance
or defensiveness. While early sessions were marked by resistance to emotional
transparency, the partners increasingly embraced the therapeutic invitation to
confront uncomfortable truths. Partner 1 reflected on this process:
"I
feel like I’ve finally been heard. I’ve been holding onto so much, and now it
feels like there’s space for us to grow." (Partner 1, session 2)
Partner 2
acknowledged a growing awareness of the need to face emotional reality to move
forward:
"It’s
hard, but I see now that I’ve been so afraid of facing the truth. I’m starting
to understand that we need to stop running from these things if we want to move
forward." (Partner 2, session 3)
This
enhanced emotional transparency was undergirded by the therapist’s consistent
enactment of radical presence and ethical strategic interventions, which modeled vulnerability
while maintaining safety and control in the therapeutic space. This approach
empowered the couple to take relational risks, knowing the therapist would
modulate the process to prevent overwhelming escalation.
As
therapy progressed, both partners began to internalize shared responsibility
for relational difficulties, moving beyond a cycle of blame. Partner 1
expressed this shift:
"I
don’t feel like I’m blaming you anymore. I see how I’ve contributed to the
mess, too." (Partner 1, session 3)
Partner 2
mirrored this acknowledgment:
"I’m
starting to believe that it’s not all on you. We’re both part of this, and
we’re both going to have to face it together." (Partner 2, session 3)
This
movement toward mutual accountability signified a pivotal breakthrough in the
systemic dynamics of their relationship and reflected the efficacy of targeted
strategic interventions disrupting maladaptive cycles.
Patient
reflections throughout therapy indicated that despite the discomfort inherent
in confronting painful emotions and entrenched patterns, they experienced
growing empowerment and hope. Partner 1 noted:
"I
used to feel like we were stuck in a loop. No matter what we said, it just felt
like we weren’t hearing each other. But now, I think I can say things that I
was afraid to say before." (Partner 1, session 3)
Similarly,
Partner 2 described an emerging confidence in vulnerability:
"I’ve
always been so scared to say the wrong thing or make it worse. But now, I feel
like I can be honest, even when it’s hard, and trust that we’ll work through
it."
(Partner 2, session 3)
While the
couple acknowledged that their relational work remained ongoing and non-linear,
the therapeutic process had effectively restructured their interactional
patterns toward increased openness, accountability, and emotional connection.
These are key markers of systemic healing within SFT.
Prognosis.
Based
on observations and progress made throughout therapy, the prognosis for the
couple is cautiously optimistic. Both partners have demonstrated the ability to
engage in vulnerable, honest
communication was a critical factor for the health and longevity of their
relationship. They have begun to acknowledge their individual contributions to
the relational dysfunction and seem motivated to continue working together
toward mutual healing.
However,
challenges remain. Despite progress, resentment, though diminished, still
lingers, and fully letting go of old emotional defenses will require time. The
couple’s history of avoidance and emotional disconnection may re-emerge during
stressful periods or conflicts. Continued commitment to open
communication and vulnerability, especially in difficult moments, will be
essential.
Given
their current trajectory, the couple is likely to continue making progress,
though the pace may vary. If they maintain commitment to utilizing therapeutic
tools and insights, they have the potential to develop a more emotionally
honest and fulfilling relationship. Periodic check-ins or follow-up sessions
may help reinforce progress and address emerging challenges.
Pre/Post
Measures. While
no formal quantitative pre/post measures were administered, the couple’s
qualitative reflections suggest significant positive change. Their capacity to
name and confront resentment, emotional avoidance, and defensiveness at
therapy’s conclusion indicates increased emotional awareness and reduced
relational dysfunction. These improvements were observable in both partners'
interactions during therapy (as indicated in Table 1), indicating an overall
positive shift in the relational dynamic.
Patient Perspective
Throughout
therapy, the couple experienced discomfort and resistance but also recognized
the necessity of the work in fostering meaningful change. As the sessions
progressed, both partners began to articulate a growing sense of agency and
emotional clarity. In earlier sessions, they described feeling trapped in
recursive loops of resentment and emotional disengagement. By the end of
therapy, however, their reflections demonstrated increased self-awareness and a
shift toward emotional responsibility.
"I
used to feel like we were stuck in a loop. No matter what we said, it just felt
like we weren’t hearing each other. But now, I think I can say things that I
was afraid to say before." (Partner 1, session 3)
This
indicated Partner 1’s movement toward greater communicative agency and a
disruption of prior avoidance patterns, consistent with the goals of strategic
pattern interruption (Haley, 1984).
"I’ve
always been so scared to say the wrong thing or make it worse. But now, I feel
like I can be honest, even when it’s hard, and trust that we’ll work through
it."
(Partner 2, session 3)
Partner
2's comment reflected a parallel shift one that moved from fear-driven silence
to engaged vulnerability, a necessary step in dismantling defensive structures
within the relationship.
These
statements reflected more than surface-level improvements as they evidenced
successful disruption of entrenched interactional patterns. The couple, once
caught in a system of blame and avoidance, began to confront their roles in the
dysfunction, a hallmark of SFT’s reframing of symptoms as systemic rather than
individual (Haley & Richeport-Haley, 2004). The therapist’s modeling of
radical honesty, coupled with structured, ethically attuned interventions
([Author], 2025a), allowed both partners to take emotional risks without
destabilizing the therapeutic process.
Importantly,
the couple no longer framed their difficulties as located in the other.
Instead, they acknowledged the relational system as the locus of dysfunction.
This shift from linear causality to circular responsibility signaled a core
epistemological shift consistent with strategic therapy’s systemic orientation
(Haley, 1987). The therapy process thus succeeded not only in symptom reduction
but in fostering a more sophisticated understanding of relational
responsibility.
Clinical Limitations
The
clinical focus in this intervention emphasized interactional sequences and
meaning-making processes over treating the presenting complaint as an isolated
or self-evident entity. Partner 1’s primary concerns “job instability and
the demands of parenthood,” were situated in the martial system as
entrenched dynamics of emotional avoidance, defensiveness, and mutual
resentment. This focus was consistent with systemic family therapy principles,
particularly efforts to disrupt recursive patterns and reframe individual
symptoms as relational phenomena (Haley, 1984; [Author], 2025a, 2025b).
However, this approach did not explicitly engage the broader gendered and
socioeconomic dimensions that Partner 1 voiced. Although these factors were
acknowledged, they remained largely peripheral to the intervention. The demands
of caregiving, labor instability, and implicit gender role expectations
especially as they intersected with power and vulnerability in the couple’s
dynamic were not substantively addressed.
This
constitutes a clinical limitation of the case, as failing to integrate these
contextual dimensions may constrain the depth and sustainability of therapeutic
change. Future systemic interventions may benefit from more deliberately
incorporating sociocultural and structural considerations into case formulation
and dialogue. Addressing how gender roles, economic precarity, and social
expectations shape relational distress can enhance both the precision and the
ethical grounding of systemic work (Carr, 2019, 2025; Perez & Karney,
2025).
Reflections
and Analytic Commentary
The
therapeutic engagement with this couple illustrates the strategic, ethically
calibrated disruption of recursive emotional patterns central to SFT. As
conceptualized by Bateson (1972), relational dysfunction emerges not from
isolated intrapsychic pathology but from homeostatic feedback loops in which
symptoms function communicatively to stabilize self-perpetuating systemic
ecology (Bateson, 1972; Broderick, 1993; Haley, 1973). The therapist’s task,
therefore, is not merely to facilitate insight but to enact epistemic
disruption—a principle foregrounded in [Author]’s (2025c) philosophical
reframing of Haley as a pragmatist of rupture rather than a collaborator of
consensus. Within this framework, the therapist operates as a directive yet
ethically accountable agent who leverages paradox, authority, and strategic
maneuvering to provoke systemic reorganization and adaptive flexibility
([Author], 2024, 2025a, 2025b).
Strategic
Disruption and the Ethics of Intervention. Throughout this case,
interventions such as strategic confrontation, prescribing the symptom, and
structured double-binds were not deployed arbitrarily but were tactically
enacted to destabilize entrenched emotional homeostasis. For example, the
reverse symptom prescription (i.e., asking the couple to intentionally avoid
each other) surfaced latent attachment needs and exposed the futility of their
defensive distancing strategies. Similarly, the double-bind (“You can stay
silent, but silence speaks too”) illuminated the recursive logic by which each
partner maintained passivity under the guise of protection. In Batesonian
terms, these maneuvers created a logical level shift, forcing the system to
confront its own governing premises.
These
interventions might, in a traditional ethical frame, be critiqued as coercive
or manipulative—a concern long associated with pure SFT (Smith et al., 2011;
Solovey & Duncan, 1992). However, as [Author] (2025c) argues, Haley’s model
is best understood as epistemology-by-intervention: the therapist enacts a
temporary, morally accountable asymmetry not to dominate, but to unsettle and
reconfigure. The goal is not consent through explanation, but transformation
through lived contradiction. When applied with relational attunement and
radical presence (McNamee, 2021), these techniques move beyond coercion into
the domain of ethically disruptive care.
Radical Honesty as
Strategic Intervention. In this case, radical honesty served as a vehicle for
both systemic confrontation and therapeutic realignment. While not formally a
Haleyan invention, radical honesty was embedded in a broader ecology of
strategic intent. Rather than inviting vulnerability for its own sake, the
therapist used honesty as a disruptive epistemic move ([Author], 2025c),
aligning with Haley’s preference for action over interpretation. This tactic
was evident in the “guided ordeal,” where each partner disclosed a
long-withheld emotional truth, not as catharsis but as a repositioning maneuver
that tested and recalibrated their relational stances.
Importantly, the
therapist’s use of radical honesty was buffered by radical presence (Lord,
2017; Shotter, 2005). This presence rendered the confrontation tolerable, if
not transformative, protecting the process from tipping into emotional
overwhelm or shame. As Bateson (1972) emphasized, the pattern that connects is
often paradoxical and nonlinear; here, strategic honesty functioned not as
content but as pattern-shifting form.
Modeling
Relational Accountability. In contrast to the passive neutrality sometimes
valorized in postmodern traditions, this case illustrated the utility of
therapist authority as ethical modeling. Through calculated asymmetry, the
therapist assumed temporary control of the system not to impose solutions, but
to expose each partner’s participation in the system’s dysfunction. By enacting
what [Author] (2025a) calls “moral asymmetry for systemic symmetry,” the
therapist compelled the couple to move from mutual blame to mutual accountability.
This shift reflected Haley’s principle that change in one part of the system
necessarily reverberates through the whole (Broderick, 1993; Haley, 1984).
Techniques
such as role repositioning and the therapist-as-problem intervention
exemplified this logic. When Partner 2 was asked to take temporary leadership
in emotional expression, the couple’s relational balance shifted. When the
therapist deliberately withheld affirmations of “progress,” the partners began
to validate one another directly—evidence that the dyadic system was becoming
self-sustaining. These moments underscored that the therapeutic relationship
functions not as mirror but as catalytic third (McNamee, 2016; Zhu, 2018).
Systemic Realignment
through Dialogical Presence. Building on Shotter’s (2005) theory of
expressive-responsive dialogue and Wittgensteinian language-games (Hintikka,
1979), the therapist’s practice of radical presence was pivotal in maintaining
relational engagement amid resistance. This stance, grounded in Batesonian
systemic epistemology, facilitated a co-constructed process of meaning-making
that repositioned the couple’s narratives from entrenched defensiveness toward
openness and connection (McNamee, 2021). Radical presence served as a moral
posture that both enabled and contained the disruptive effects of strategic
interventions, underscoring the inseparability of clinical pragmatism and
ethical commitment.
Navigating
Feedback, Non-Linearity, and Setback. The couple’s journey toward
emotional vulnerability did not proceed linearly. Moments of rupture followed
breakthroughs, and periods of progress were punctuated by defensive
regressions. This oscillation is not pathological; it reflects the systemic principle
that change begets resistance and that systems often revert to homeostasis
before stabilizing at a new level of functioning (Barman et al., 2022; Bateson,
1972). The therapist’s role in this ecology was not to pathologize setbacks,
but to contextualize them within a recursive feedback framework—what [Author]
(2025c) might term an "ecology of epistemic disruption."
Indeed,
each recurrence of avoidance provided new data for the system to reorganize.
The therapist normalized these fluctuations, thereby disarming their power to
stall progress. In this way, therapy enacted a pragmatist ethics (Dewey, 1938;
Kolb, 2015), where meaning is generated not through linear insight but through
lived, iterative experimentation.
Addressing
Critiques of Coercion and Power. Finally, it is critical to situate these
interventions within broader debates about the ethics of power in therapy. As
[Author]’s (2025c) analysis and Table 2 highlight, critics have long flagged
SFT’s strategic techniques as potentially manipulative or culturally
insensitive. However, this case aligns with a newer tradition of postmodern
derivatives (e.g., Madanes, 1990; Sexton, 2019; Szapocznik et al., 2015) that
preserve Haley’s systemic rigor while reconfiguring authority as dialogical
responsibility rather than strict hierarchical control.
In
this model, therapist authority is exercised not to dictate but to initiate
contradiction; and, thus, provoke the family system into confronting its own
incoherencies. This is epistemology not as static knowledge but as
feedback-informed reorganization, as Haley (1984) himself insisted. Properly
wielded, such strategic interventions are not coercive, but catalytic provided
they are embedded in relational ethics, ecological sensitivity, and
moment-to-moment attunement.
Conclusion
SFT,
when understood as modernist-pragmatism, grounded in Batesonian systemic
epistemology, emerges not as a relic of hierarchical manipulation, but as a
philosophically coherent, ethically accountable framework for clinical change.
This case demonstrates how strategic confrontation, radical honesty, and
systemic disruption, when enacted with relational presence and moral intent,
can facilitate the dismantling of rigid interactional patterns and promote
sustainable relational transformation. The therapist does not merely guide
change they provoke possibility within the ecology of mind.
Ethical
Considerations
Informed
consent was obtained prior to therapy initiation, ensuring confidentiality and
both partners’ understanding of the research purposes. Data handling complied
with ethical research standards, drawing on multiple case reporting frameworks:
the CARE guidelines (Gagnier et al., 2013), the psychotherapy-specific
standards of Eells (2022), and the CaSE tool (Kaluzeviciute, 2021). Ethical
practice was further grounded in the AAMFT Code of Ethics (2015), specifically
Principle I (responsibility to clients: informed consent and confidentiality)
and Principle III (professional competence and integrity).
This
case study was conducted within a systemic psychotherapy practice as part of
routine clinical work rather than as experimental research; therefore, it was
not subject to formal Institutional Review Board approval, in accordance with
prevailing standards for single-case reports that do not extend beyond usual
care (International Committee of Medical Journal Editors [ICMJE], 2022). The
study was assessed as minimal risk, as no procedures extended beyond standard
therapeutic practice. Both partners provided written informed consent for
participation and for publication of fully de‑identified clinical
material.
Data Availability
Statement
The
data supporting the results of this case study are not publicly available due
to privacy concerns. Specific details, including codebook, regarding the case
study are available upon reasonable request from the corresponding author
Funding
This
research was funded by Easy Does It Counseling, P.C., a nonprofit 501(c)(3)
organization operating across multiple states in the United States.
Competing Interests
The author is the founding CEO and clinical
director of Easy Does It Counseling. No known financial or commercial conflicts
of interest related to this research are declared.
Use of AI technologies
The
author confirms that no generative AI tools were used in the conception,
drafting, analysis, interpretation, or revision of this manuscript.
References
Almeida, B., & Cunha, C. (2023). Time, resentment, and
forgiveness: Impact on the well-being of older adults. Trends in Psychology,
1–20. https://doi.org/10.1007/s43076-023-00343-2
American Association for Marriage and Family Therapy [AAMFT].
(2015). Code of ethics. https://www.aamft.org/AAMFT/Legal_Ethics/Code_of_Ethics.aspx
Andersen, T. (1991). The reflecting team: Dialogues and
dialogues about the dialogues. W. W. Norton.
Anderson, C., & Erstling, S. S. (1983). Common problems in
application. In R. F. Luber & C. Anderson (eds.), Family Therapy with
Psychiatric Patients (pp. 121–137). Human Sciences Press.
Angus, L. E., & Greenberg, L. S. (2011). Working with
narrative in emotion-focused therapy: Changing stories, healing lives.
American Psychological Association. https://doi.org/10.1037/12325-000
Angus, L. E., & McLeod, J. (2004). The handbook of narrative
and psychotherapy: Practice, theory, and research. Sage Publications.
Asen, E. (2002). Outcome research in family therapy. Advances in
Psychiatric Treatment, 8(3), 230–238. https://doi.org/10.1192/apt.8.3.230
Barman, J. D., Maheshwari, S., & Varma, P. (2022). The
conflicts and conflict management in stable middle-class marriages: An Indian
perspective. The Family Journal. https://doi.org/10.1177/10664807221124231
Bateson, G. (1972). Steps to an ecology of mind: Collected
essays in anthropology, psychiatry, evolution, and epistemology. University
of Chicago Press.
Bobrow, E., & Ray, W. A. (2005). Strategic family therapy in
the trenches. Journal of Systemic Therapies, 23(4), 28–42. https://doi.org/10.1521/jsyt.23.4.28.57840
Bolton, G. (2010). Reflective practice: Writing and professional
development (3rd ed.). SAGE Publications.
Boscolo, L., Cecchin, G., Hoffman, L., & Penn, P. (1987). Milan
systemic family therapy: Conversations in theory and practice. Basic Books.
Braun, V., & Clarke, V. (2006). Using thematic analysis in
psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Broderick, C. B. (1993). Understanding family process: Basics of
family systems theory. Sage.
Brown, J. M. (2012). The Milan principles of hypothesising,
circularity and neutrality in dialogical family therapy: Extinction, evolution,
eviction… or emergence? Australian and New Zealand Journal of Family
Therapy, 31(3), 248–265. https://doi.org/10.1375/anft.31.3.248
Brothers, B. J. (1993). Make love not war—or at least make meaning.
Journal of Couples Therapy, 3(4), 1–6. https://doi.org/10.1300/J036v03n04_01
Bruner, J. (1990). Acts of meaning. Harvard University
Press.
Carlson, C. I., Ross, S. G., & Stark, K. H. (2012). Bridging
systemic research and practice: Evidence-based case study methods in couple and
family psychology. Couple and Family Psychology: Research and Practice, 1(1),
48–60. https://doi.org/10.1037/a0027511
Carr, A. (2019). Couple therapy, family therapy and systemic
interventions for adult‐focused problems: The current evidence base. Journal
of Family Therapy, 41(4), 492–536. https://doi.org/10.1111/1467-6427.12225
Carr, A. (2025). Couple therapy and systemic interventions for
adult‐focused problems: The evidence base. Journal of Family Therapy, 47(1),
e12481. https://doi.org/10.1111/1467-6427.12481
Daneshpour, M. (2024). Couples therapy and the challenges of
building trust, fairness, and justice. Family Process, 1–15. https://doi.org/10.1111/famp.13072
de Shazer, S. (1985) Keys to solutions in brief therapy. W.
W. Norton.
de Shazer, S. (1988) Clues: Investigating solutions in brief
therapy. W. W. Norton.
de Shazer, S., & Berg, I. K. (1997). ‘What works?’ Remarks on
research aspects of solution‐focused brief therapy. Journal of Family
Therapy, 19(2), 121–124.
Dewey, J. (1938). Experience and education. Macmillan
Company.
Donkoh, S., & Mensah, J. (2023). Application of triangulation
in qualitative research. Journal of Applied Biotechnology and
Bioengineering, 10(1), 6–9. https://doi.org/10.15406/jabb.2023.10.00319
Finlay, L. (2002). “Outing” the researcher: The provenance,
process, and practice of reflexivity. Qualitative Health Research, 12(4),
531–545. https://doi.org/10.1177/104973202129120052
Gagnier, J. J., Kienle, G., Altman, D. G., Moher, D., Sox, H.,
& Riley, D. (2013). The CARE guidelines: Consensus-based clinical case
reporting guideline development. Journal of Clinical Epidemiology, 67(1),
46–51. https://doi.org/10.1016/j.jclinepi.2013.08.003
Greenberg, L. S. (1988). Emotionally focused therapy for
couples. Guilford Press.
Greenberg, L. S. (2010). Emotion-focused therapy: A clinical
synthesis. Focus, 8(1), 32–42. https://doi.org/10.1176/foc.8.1.foc32
Haley, J. (1958). The art of psychoanalysis. Et Cetera, 15(3),
190–200.
Haley, J. (1959). An interactional description of schizophrenia. Psychiatry,
22(4), 321–332. https://doi.org/10.1080/00332747.1959.11023187
Haley, J. (1973). Uncommon therapy: The psychiatric techniques
of Milton H. Erickson MD. W. W. Norton.
Haley, J. (1984). Ordeal therapy. Jossey-Bass.
Haley, J. (1993). Uncommon therapy: The psychiatric techniques
of Milton H. Erickson, M.D. W. W. Norton.
Haley, J., & Erickson, M. H. (1959). Hypnosis and therapeutic
consent: Ethical implications in clinical practice. American Journal of
Clinical Hypnosis, 2(2), 49–84.
Hargaden, H., & Sills, C. (2014). Transactional analysis: A
relational perspective. Routledge. https://doi.org/10.4324/9781315820279
Harris, R. (1990). Language, Saussure and Wittgenstein: How to
play games with words. Psychology Press.
Hedges, F. (2005). An introduction to systemic therapy with
individuals: A social constructionist approach. Palgrave Macmillan.
Hintikka, J. (1979). Language-games. In E. Saarinen (ed.), Game-Theoretical
Semantics: Essays on Semantics by Hintikka, Carlson, Peacocke, Rantala, and
Saarinen (pp. 1–6). Springer Netherlands. https://doi.org/10.1007/978-1-4020-4108-2_1
International Committee of Medical Journal Editors [ICMJE]. (2022).
Recommendations for the conduct, reporting, editing, and publication of
scholarly work in medical journals. Retrieved from http://www.icmje.org/
Jockers, M. L., & Thalken, R.
(2020). Text analysis with R: For students of literature (2nd ed.).
Springer. https://doi.org/10.1007/978-3-030-39643-5
Johnson, S. M. (2004). The practice of emotionally focused
couple therapy: Creating connection (2nd ed.). Brunner-Routledge.
Johnson, S. M., & Greenberg, L. S. (1985). Differential effects
of experiential and problem-solving interventions in resolving marital
conflict. Journal of Consulting and Clinical Psychology, 53(2), 175–184.
https://doi.org/10.1037/0022-006X.53.2.175
Johnson, S. M., & Greenberg, L. S. (1987). Emotionally focused
marital therapy: An overview. Psychotherapy: Theory, Research, Practice,
Training, 24(3S), 552–560. https://doi.org/10.1037/h0085753
Kolb, D.A. (2015). Experiential learning: Experience as the
source of learning and development (2nd ed.). Pearson.
Krippendorff, K. (2018). Content analysis: An introduction to
its methodology (4th ed.). Sage Publications.
[Author]. (2024). Increasing transgender acceptance in religious
families: A pilot study of manualized strategic family therapy. International
Journal of Systemic Therapy, 36(1), 1–34. https://doi.org/10.1080/2692398X.2024.2408135
[Author]. (2025a). Jay Haley’s ethical legacy: Bioethics, family
therapy, and the AAMFT code. History and Philosophy of Medicine, 7(3),
15. https://doi.org/10.53388/HPM2025015
[Author]. (2025b). Review of ‘Strategies of Psychotherapy.’
ScienceOpen. https://doi.org/10.14293/S2199-1006.1.SOR-UNCAT.BKNHO5.v1.RPIIEL
[Author] (2025c). Jay Haley’s model of strategic family therapy: An
epistemological inquiry. Philosophy, Psychiatry, & Psychology.
Advanced online publication. https://doi.org/10.1353/ppp.0.a971258
Lord, S. (2017). Mindfulness, intimacy, and presence: Moments of
meeting in psychotherapy. In S. Lord (Ed.), Moments of Meeting in
Psychoanalysis: Interaction and Change in the Therapeutic Encounter (pp.
358–374). Routledge. https://doi.org/10.4324/9781315389967
McLeod, J. (2011). Qualitative research in counselling and
psychotherapy (2nd ed.). Sage Publications.
McNamee, S. (2016). The ethics of relational process: John
Shotter’s radical presence. In Joint action (pp. 101–113). Routledge.
McNamee, S. (2020). Radical presence: Alternatives to the
therapeutic state. In D. Loewenthal, O. Ness, & B. Hardy (Eds.), Beyond
the Therapeutic State (pp. 55–65). Routledge.
McNamee, S. (2021). Radical presence: A relational alternative to
mindfulness. In R. Aristegui, J. G. Campayo, P. Barriga (Eds.), Relational
Mindfulness: Fundamentals and Applications (pp. 51–63). Routledge.
McNamee, S., & Shawver, L. (2004). Therapy as social
construction: Back to basics and forward toward challenging issues. In T.
Strong, & D. Paré (Eds.), Furthering Talk: Advances in the Discursive
Therapies (pp. 253–270). Springer.
Minuchin, S. (1974). Families and family therapy. Harvard
University Press.
Minuchin, S. (2007). Jay Haley: My teacher. Family Process,
46(3), 413–414. https://doi.org/10.1111/j.1545-5300.2007.00220.x
Morales, E. (2020). Mindfulness as an embodied relational resource
in generative dialogue. In A. Arnold, K. Bodiford, P. Brett-MacLean, D. Dole,
A. M. Estrada, F. L. Dugin, B. Milne, W. E. Raboin, P. Torres-Dávila, & C.
F. Villar-Guhl (Eds.), Social Construction in Action (pp. 126–134). Taos
Institute Publications.
Perez, J. C., & Karney, B. R. (2025). Financial strain and
couple relationships: Acknowledging the material challenges of couples living
with low socioeconomic status. In N. C. Overall, J. A. Simpson, & J. A.
Lavner (Eds.), Research Handbook on Couple and Family Relationships (pp.
298–313). Edward Elgar Publishing. https://doi.org/10.4337/9781035309269
Roddy, M. K., Walsh, L. M., Rothman, K., Hatch, S. G., & Doss,
B. D. (2020). Meta-analysis of couple therapy: Effects across outcomes,
designs, timeframes, and other moderators. Journal of Consulting and
Clinical Psychology, 88(7), 583–596. https://doi.org/10.1037/ccp0000493
Roth, S., & Epston, D. (1998). Consulting the problem about the
problematic relationship: An exercise for experiencing a relationship with an
externalized problem. In M. F. Hoyt (Ed.), Constructive Therapies (Vol.
2; pp. 148–162). Guilford Press.
Small, M. L., Brant, K., & Fekete, M. (2024). The avoidance of
strong ties. American Sociological Review, 89(4), 615–649. https://doi.org/10.1177/00031224241263602
Shotter, J. (2005). ‘Inside the moment of managing”: Wittgenstein
and the everyday dynamics of our expressive-responsive activities. Organization
Studies, 26(1), 113–135. https://doi.org/10.1177/0170840605049718
Solovey, A. D., & Duncan, B. L. (1992). Ethics and strategic
therapy: A proposed ethical direction. Journal of Marital and Family
Therapy, 18(1), 53–61. https://doi.org/10.1111/j.1752-0606.1992.tb00914.x
Spengler, P. M., Lee, N. A., Wiebe, S. A., & Wittenborn, A. K.
(2024). A comprehensive meta-analysis on the efficacy of emotionally focused
couple therapy. Couple and Family Psychology: Research and Practice, 13(2),
81–99.
Stake, R. E. (1995). The art of case study research. Sage
Publications.
Stake, R. E. (2013). Qualitative research: Studying how things
work. Guilford Press.
Vetere, A., & Stratton, P. (2016). Interacting selves:
Systemic solutions for personal and professional development in counselling and
psychotherapy. Routledge.
Villa, V. (2024). A joint endeavour: Working with couples. In E.
Haynes (Ed.), A Transactional Analysis of Motherhood and Disturbances in the
Maternal (1st ed., pp. 242–258). Routledge. https://doi.org/10.4324/9781003365822
Vos, J., & van Rijn, B. (2021). The evidence-based conceptual
model of transactional analysis: A focused review of the research literature. Transactional
Analysis Journal, 51(2), 160–201. https://doi.org/10.1080/03621537.2021.1904364
White, M., & Epston, D. (1990). Narrative means to
therapeutic ends. W. W. Norton.
Williams, B. C. (2016). Radical honesty: Truth-telling as pedagogy
for working through shame in academic spaces. In F. Tuitt, C. Haynes, & S.
Stewart (Eds.), Race, Equity, and the Learning Environment: The Global
Relevance of Critical and Inclusive Pedagogies in Higher Education (pp.
71–82). Routledge.
Wilner, R. S., Breit, M., & Im, W. G. (1988). In defense of
strategic therapy. Contemporary Family Therapy, 10(3), 169–182. https://doi.org/10.1007/BF00895619
Wittenborn, A. K., Liu, T., Ridenour, T. A., Lachmar, E. M.,
Mitchell, E. A., & Seedall, R. B. (2018). Randomized controlled trial of
emotionally focused couple therapy compared to treatment as usual for
depression: Outcomes and mechanisms of change. Journal of Marital and Family
Therapy, 45(3), 395–409. https://doi.org/10.1111/jmft.12350
Zhu, J. (2018). "We're not cheaters": Polyamory,
mixed-orientation marriage and the construction of radical honesty. Graduate
Journal of Social Science, 14(10), 57–78.